Article Text

Statistics from Altmetric.com
Description
A 25-year-old man with no significant medical or surgical history presented with a complaint of thick, dark drainage from a periumbilical wound for 1 month (figure 1). He reported first noticing the drainage several days after bumping into the corner of a machine at work. He was seen by his primary care physician and prescribed oral antibiotics for persistent drainage and erythema; however, his symptoms failed to improve.

Chronic umbilical wound sustained after blunt abdominal trauma, with drainage of a thick, dark fluid for 1 month.
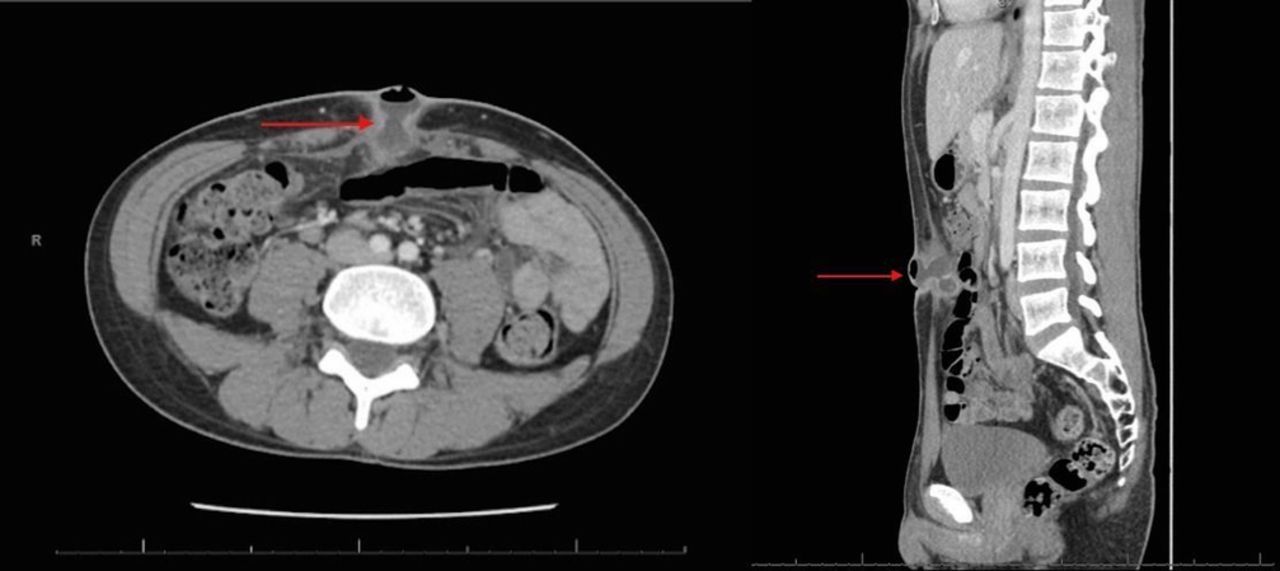
On presentation to the emergency department, the patient was afebrile and haemodynamically stable. Lab work was within normal limits. An abdominal CT scan demonstrated a loculated periumbilical fluid collection, with extension intraperitoneally into a portion of thickened small bowel with suspicion of an enterocutaneous fistula (figure 2).
{kind=link}
{kind=link}
Loculated periumbilical fluid collection approximately 3.8×2.2×3.4 cm. An intraperitoneal portion of the fluid collection is contiguous with a thickened small bowel loop, which is suspicious for an enterocutaneous fistula.
The decision was made to take the patient to the operating theatre for further examination. Intraoperatively, the presence of a loop of small bowel densely adherent to the umbilicus was identified. After careful dissection, there appeared to be a perforated diverticulum located in proximity to the ileocaecal junction. The edges of the surrounding bowel were noted to be necrotic, and the decision was made to resect the segment. A small bowel resection was performed with primary anastomosis. The remainder of the patient’s hospital course was uncomplicated. Surgical pathology confirmed a 2.5 cm Meckel’s diverticulum: small intestine with a single diverticulum showing extensive mural gastric and pancreatic tissue. Histology demonstrated normal mucosa without evidence of dysplasia or autodigestion. This suggests diverticular rupture secondary to mechanical force.
Meckel’s diverticulum is an outpouching of the small intestine that results from incomplete closure of the vitelline duct. It is most commonly located 40–60 cm from the ileocaecal valve, and occurs in 2%–3% of the population.1 2 In most instances Meckel’s diverticulum is benign, asymptomatic and often diagnosed incidentally during laparoscopy/laparotomy. Meckel’s diverticulum may contain gastric or pancreatic mucosa, which can become symptomatic. Most commonly, patients with ectopic gastric mucosa form adjacent ulcers, which present as a painless lower gastrointestinal bleed.2
Traumatic rupture of a Meckel’s diverticulum is a rare occurrence. Previous cases have described rupture secondary to blunt injury from motor vehicle accidents and contact sports (soccer, softball). The force of impact during these injuries was significant enough to cause acute rupture of the diverticulum as well as arterial avulsion. These patients presented with acute signs of peritonitis, including guarding, rigidity and haemodynamic instability.1 3 A proposed aetiology for this rupture to occur is due to the sudden increase in intra-abdominal pressure. As compression of organs occurs against the impacting object and vertebrae, increased intra-abdominal pressure may cause perforation in susceptible areas such as the ileum, rectum and blind loops.3
These acute physical exam findings were absent in our patient. This is the first case reporting a blunt traumatic rupture of a Meckel’s diverticulum that presented as a chronic enterocutaneous fistula. It emphasises the importance of obtaining a thorough history and physical exam, along with proper imaging, to guide the formulation of an accurate diagnosis and treatment plan.
Learning points
Meckel’s diverticulum is often asymptomatic and discovered incidentally.
The most common presenting symptom is gastrointestinal bleeding, and this is usually secondary to gastric mucosa present within the diverticulum, resulting in an acid-induced ulcer adjacent to the diverticulum.2
Traumatic small bowel injuries are most common after blunt traumas (ie, motor vehicle accidents/seat belts, contact sports), and result in an increase in intra-abdominal pressure, which can lead to perforation in susceptible regions such as in the diverticulum or the terminal ileum.1 3
The mainstay of treatment in symptomatic and traumatic Meckel’s diverticulum is diverticulectomy, with or without bowel resection.
Resection of asymptomatic diverticulum remains controversial, and the risks/benefits and overall health of the patient must be considered.2
Footnotes
Contributors DL, KB: research, writing, editing, formatting. DL, KB, SK: final editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.