Article Text

Statistics from Altmetric.com
Description
A 34-year-old African woman, whose medical history was unremarkable, presented to the emergency room with severe headache and vomiting. Temperature, blood cells count, plasma electrolytes and chest X-ray were normal. Clinical conditions were rapidly deteriorating and neurological exam disclosed drowsiness, opisthotonus and decerebrate response to pain. Brain CT scan showed a ‘full’ posterior fossa, mild supratentorial hydrocephalus and herniation of cerebellar tonsils: after contrast, a nodule with ring enhancement and conspicuous perilesional oedema was disclosed in the right cerebellar hemisphere.
The patient was given diuretics and steroids with no success. Since the neurological conditions were worsening, a neurosurgical operation was then performed in emergency: posterior fossa was decompressed, the cerebellar nodular lesion was removed en bloc with microsurgical technique and a transient ventricular drain was placed. Neurological conditions promptly recovered after surgery.
Possible differential diagnosis:
Metastasis
Pyogenic abscess
Primitive brain tumour
Abscess from non-pyogenic agents.
Acute cerebellar tonsillar herniation determines brainstem compression and is a life-threatening condition requiring a quick neurosurgical procedure. When the cause is a supratentorial expanding mass (tumour, haematoma or hydrocephalus) the signs of intracranial hypertension come first: the patient would suffer from headache and vomiting and papilloedema is observed at ophthalmological exam; as a secondary effect of such intracranial hypertension, cerebellar tonsils and brainstem might be downward displaced through the foramen magnum with consequent decerebrate rigidity, bradycardia, arterial hypertension and apnoea.
On the contrary, if the expanding mass develops quite rapidly in the posterior fossa the brainstem compression would occur before intracranial hypertension evolves: this is the reason why in the present case we performed emergent posterior fossa decompression instead of simple ventriculostomy. The neurological exam is of paramount importance and, in particular, is important to recognise early the signs of impending brainstem compression that might develop before the clinical syndrome of intracranial hypertension: vomiting may be common to both conditions; neck stiffness and opisthotonus, instead, as well as decerebrate response to pain and Cushing reflex demonstrate a brainstem involvement.
Infratentorial lesions at risk for a direct brainstem compression may be of various origin: spontaneous (cerebellar haematoma or ischaemia), traumatic (cerebellar contusion, epidural haematoma), neoplastic (metastasis or primitive brain tumour), infective (abscess).
In the present case, the image (figure 1) depicted at CT scan, a small lesion with ring enhancement surrounded by conspicuous oedema, was consistent with both abscess and metastasis: in fact, CT features of abscess, whatever the aetiology, are non-specific. MRI would have clarified the diagnosis, but it was hampered by the rapid neurological decline.
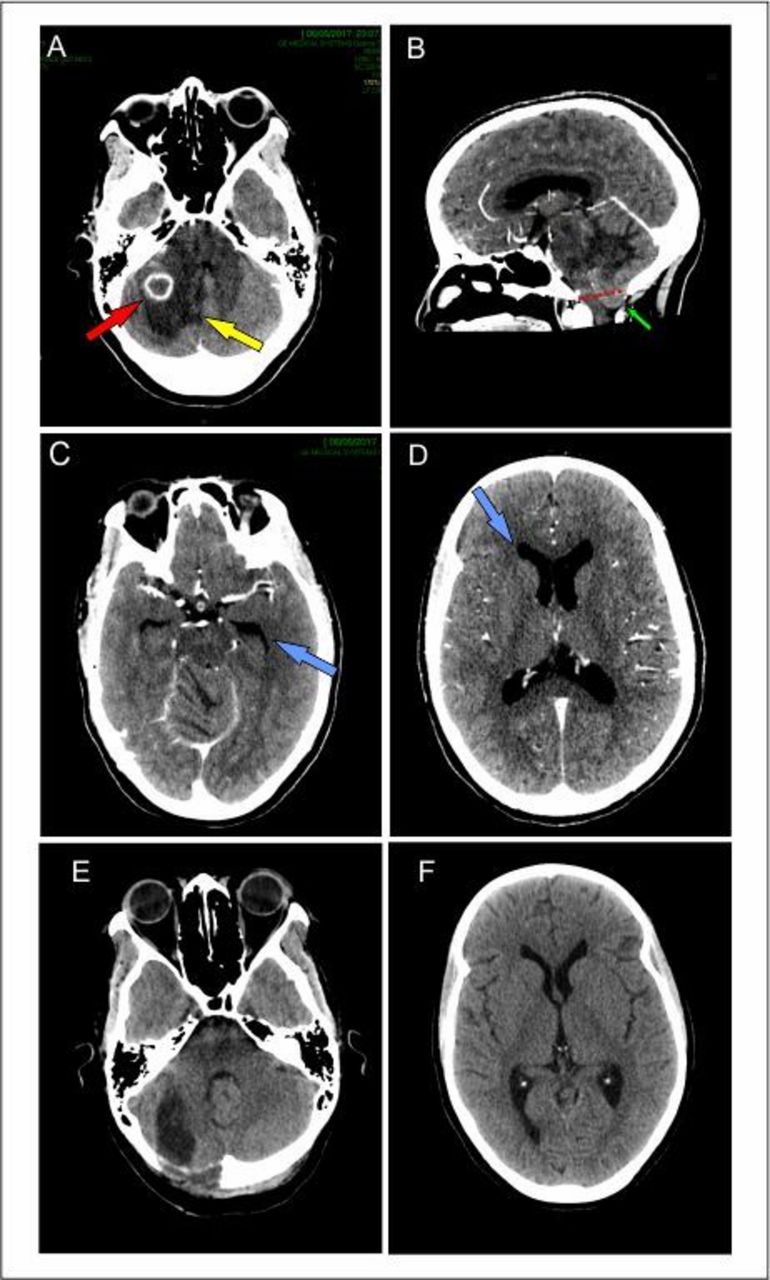
Brain CT. (A–D) Contrast-enhanced preoperative scan. (E, F) Non-contrast postoperative scan. (A) Small nodule with ring enhancement (red arrow) and massive oedema (yellow arrow). (B) Cerebellar tonsils (green arrow) herniated through the foramen magnum (red dotted line). (C) Dilated temporal horns as sign of early-stage hydrocephalus (blue arrow). (D) Mild dilatation of frontal horn (blue arrow), body and trigone of lateral ventricles. (E) Removal of abscess. (F) Slight reduction of ventricular system.
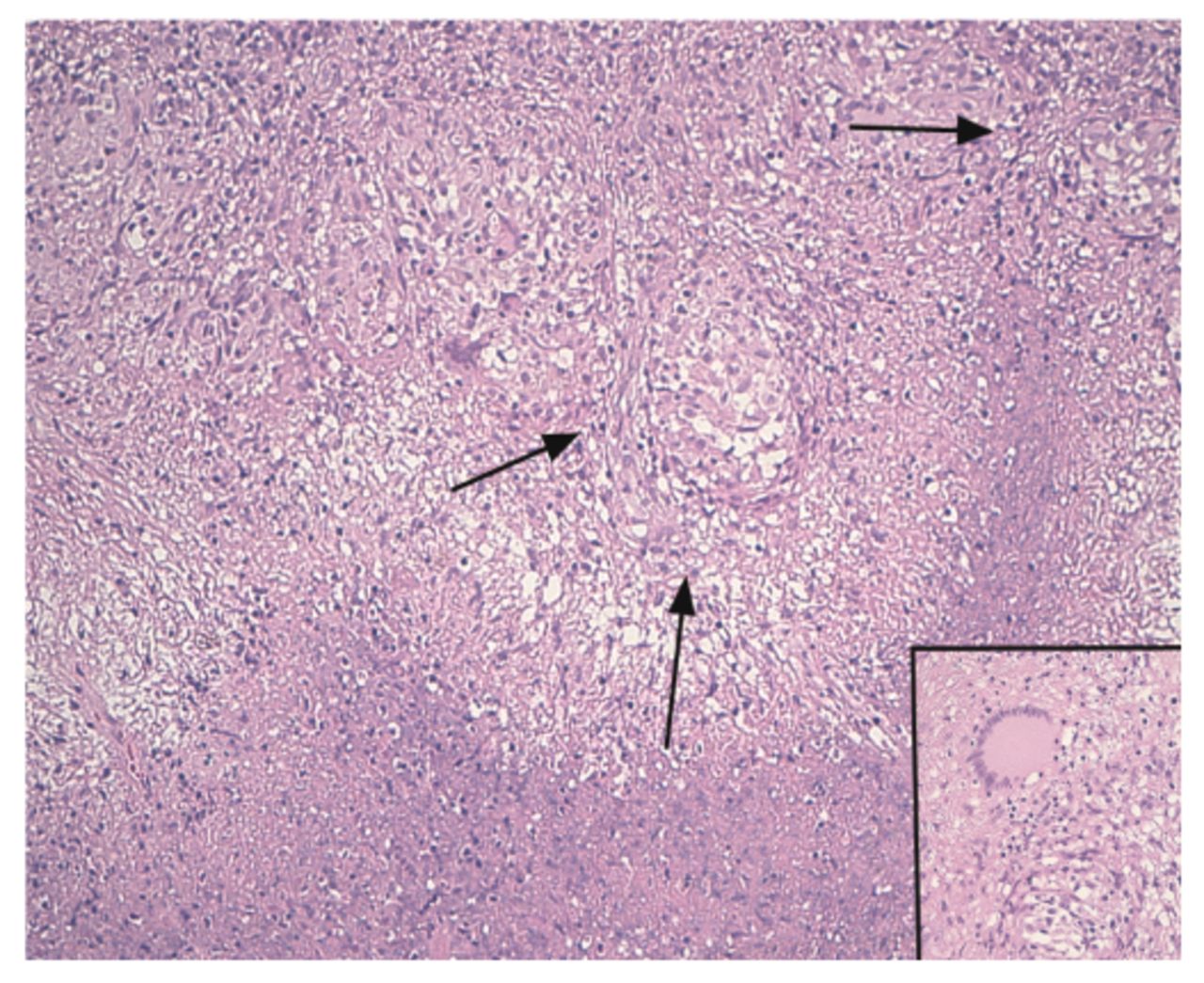
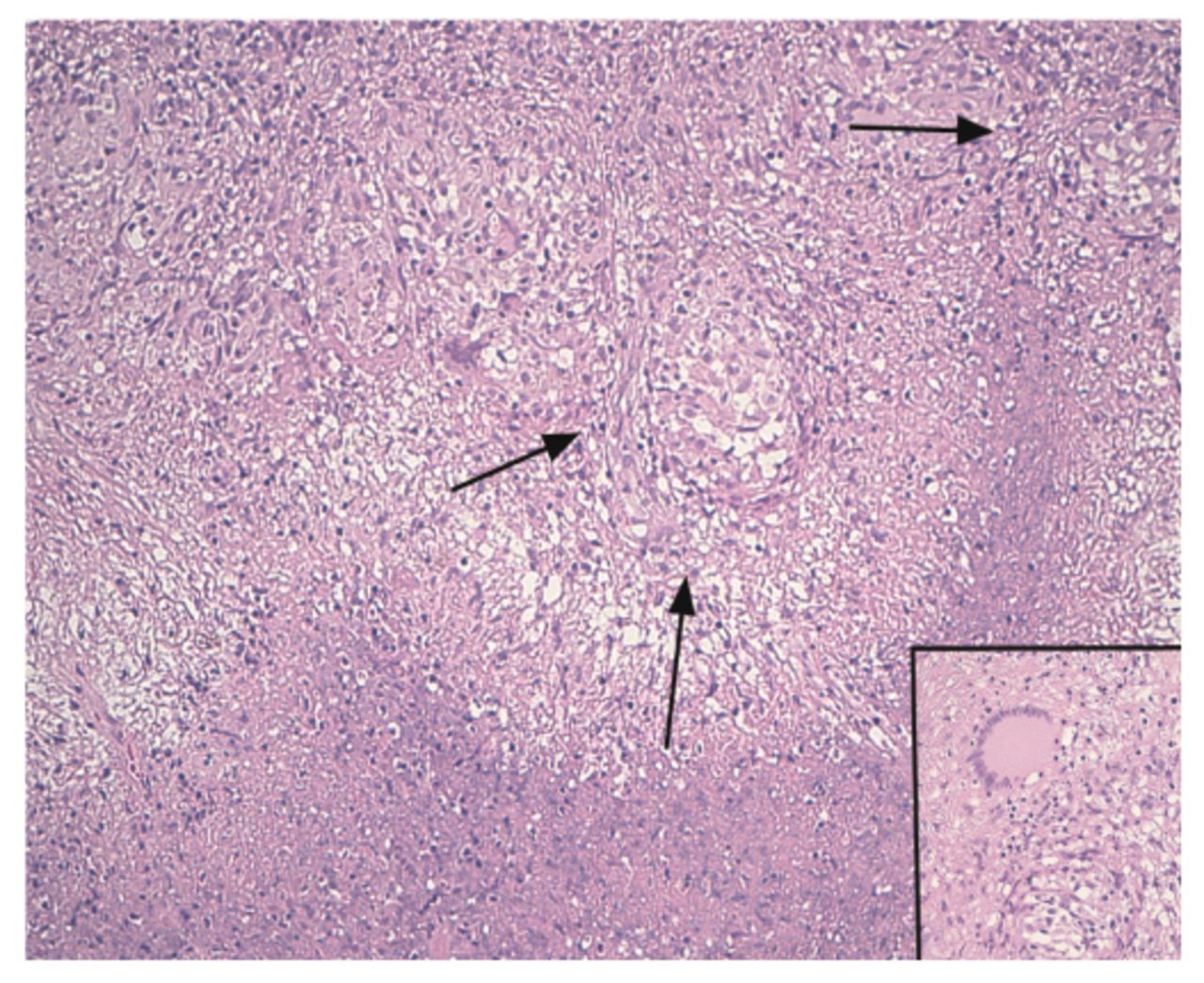
Surgery allowed a fast neurological recovery and diagnosis as well. In fact, histopathology (figure 2) recognised a granulomatous process with giant cells and on surgical specimen the Mycobacterium spp genome was identified (PCR): therefore, the diagnosis was tuberculosis. The patient was then assigned to the infection disease department where the treatment with isoniazid, rifampicin, ethambutol and pyrazinamide was started.
{kind=link}
{kind=link}
Histology. Inflammatory necrotising process with multiple microgranulomas (arrows) and Langhans-type multinucleated giant cells (inset).
Learning points
Acute brainstem compression should be promptly and correctly diagnosed.
Acute brainstem compression often requires urgent surgery.
Tubercular cerebral abscess may be the first clinical sign of tuberculosis.
Footnotes
Contributors LL: concept and design. QGDA and MG: acquisition of data and analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.