Article Text

Statistics from Altmetric.com
Description
Electrocardiographic changes in asymptomatic individuals may be a diagnostic challenge. The knowledge and early identification of these patterns and their correct association with clinical picture shall have an urgent and specific management.
A 75-year-old Caucasian man with medical history of hypertension and peripheral arterial disease presented at the emergency department, transported by the prehospital emergency team, complaining of an intense chest pain, which woke him up, with irradiation to the left upper limb and diaphoresis. The patient denied nausea, vomiting, palpitations and previous complaints of angina as well. It was administered, during transport, sublingual nitroglycerine, with resolution of the pain.
The patient was vigil, oriented and haemodynamically stable. Physical examination was unremarkable.
The admission ECG, without pain, showed sinus rhythm, heart rate of 60 bpm, right bundle branch block pattern and deep negative symmetrical T waves in the precordial derivations (V2 to V6) suggestive of type 2 Wellens’ pattern (figure 1). Blood tests documented a mild elevation of troponin I (1.76 ng/mL (normal <0012 ng/mL)), without other abnormalities.
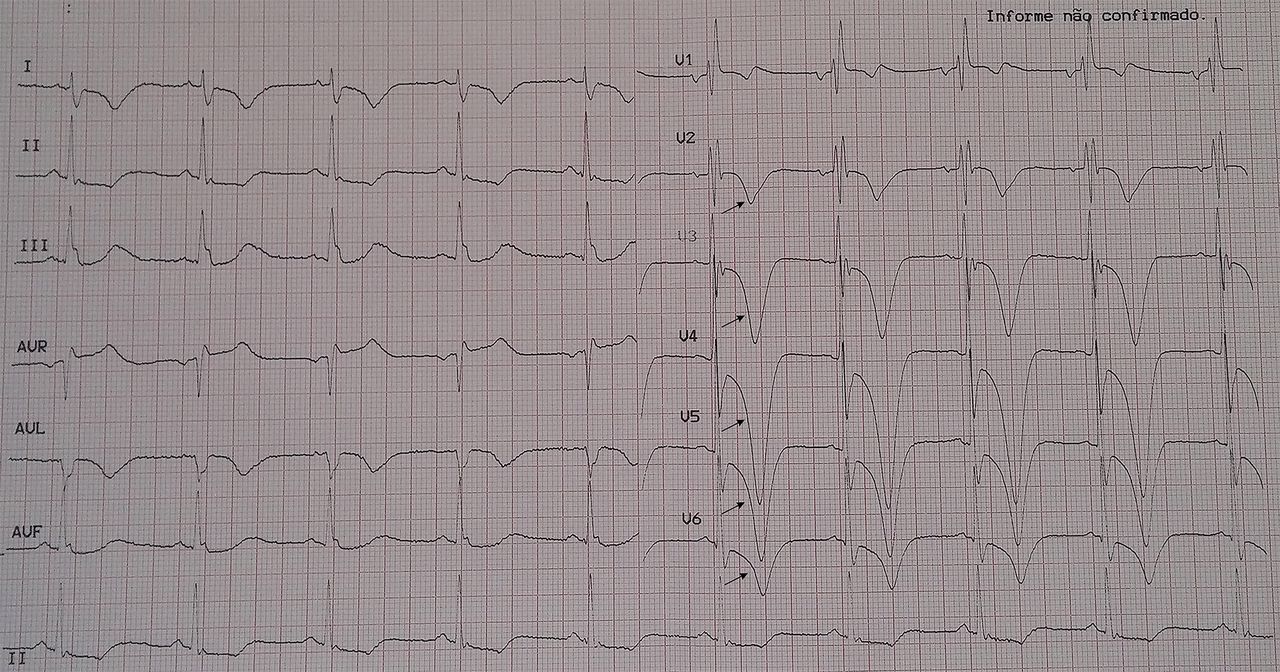
Hospital admission ECG, without chest pain, showing sinus rhythm, heart rate of 60 bpm, right bundle branch block pattern and deep negative symmetrical T waves in the precordial derivations V2 to V6 (arrow)—type 2 Wellens’ pattern.
The patient was admitted to the coronary intensive care unit with the diagnosis of acute coronary syndrome without ST-elevation.
During hospital stay, patient complained of chest pain. A new ECG was performed showing sinus rhythm, heart rate of 70 bpm, right bundle branch block pattern, no changes in ST segment and biphasic T waves in V3 (figure 2). The echocardiogram revealed mid-apical segment hypokinesia of the anterior wall conditioning mild depressed global systolic function with an estimated ejection fraction of 49%.

{kind=link}
{kind=link}
ECG performed during recurrent chest pain showing sinus rhythm, heart rate of 70 bpm, right bundle branch block pattern (arrow), no changes in ST segment and biphasic T waves in V3 (arrowhead).
Cardiac catheterisation documented a stenosis of 99% of the proximal segment of the left anterior descending (LAD) coronary artery. Angioplasty was performed with placement of one drug-eluting stent. The patient improved rapidly and was discharged home at fourth day of hospital admission.
Wellens’ syndrome was fist described by Zwann and Wellens in 1982 in a subgroup of patients with substantial risk of develop anterior myocardial infarction.1 2 This syndrome is characterised by T wave abnormalities in the anterior chest leads and reflects a critical obstruction in the proximal LAD coronary artery.1–3
The clinical, laboratorial and ECG criteria for Wellens’ syndrome is a history of angina, minimal or no elevation of cardiac enzymes, minimal or no ST-segment elevation (<1 mm), no pathological precordial Q waves and biphasic T waves in leads V2 and V3 (type 1) or deep, symmetrical and inverted T waves in leads V2 and V3, occasionally V1, V4, V5 and V6 (type 2).1 2
In a symptomatic patient, T abnormalities can normalise or evolve into ST-segment elevation.1 2
The ECG shall be the only indication of an imminent massive anterior infarction.2 So, a timely diagnostic and therapeutic approach will be able to prevent a massive infarction in LAD coronary artery territory1–3 and reduce the high morbidity and mortality associated with coronary artery disease.
Learning points
Wellens’ syndrome is characterised by T wave abnormalities in the anterior chest leads and reflects a critical obstruction in the proximal left anterior descending coronary artery.
In the symptomatic patient, T changes can normalise or evolve into ST-segment elevation.
Prompt diagnosis and therapeutic management will prevent a massive anterior myocardial infarction.
Footnotes
Contributors Conception and design of the work; data collection and analysis: TGR. Drafting the article: TGR, JP and BCP. Critical revision of the article: JP, JS and BCP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.