Article Text

Statistics from Altmetric.com
Description
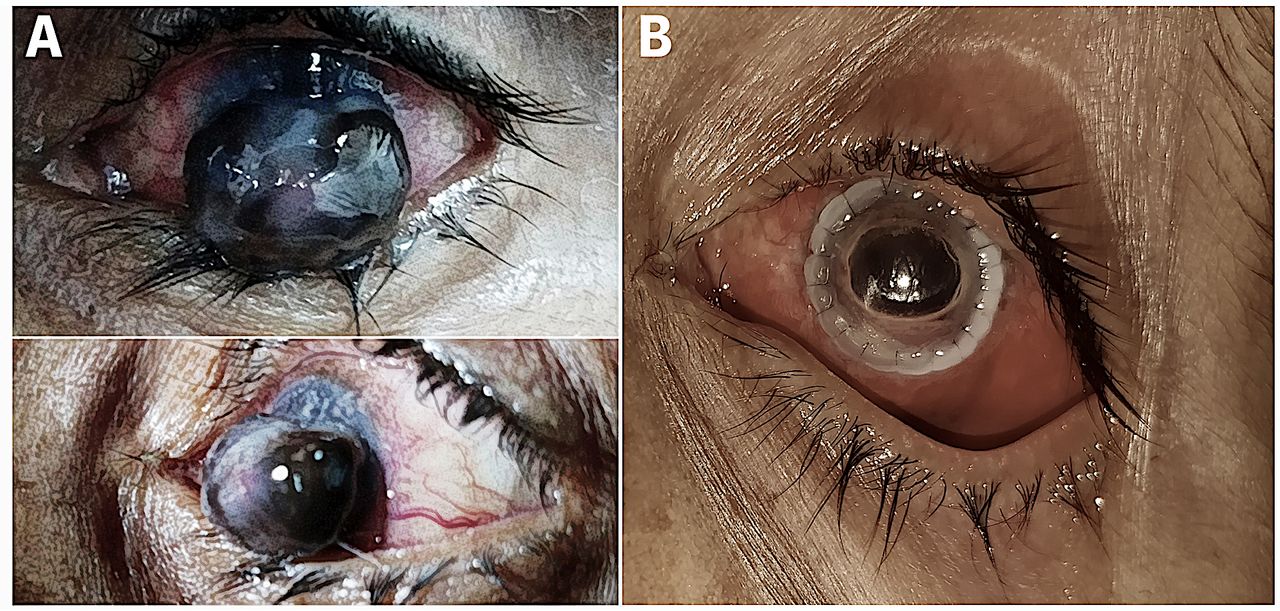
A 51-year-old woman presented to the ophthalmology emergency room with inability to close the eyelid, severe pain and light sensitivity in the left eye. Ocular examination showed severe conjunctival injection, deep corneal vascularisation, and extremely thin and protruded cornea, measuring 12×14 mm, with iridocorneal adhesions (figure 1A). The protruded lesion had a typical blueberry-like external appearance, due to the iris plugging the perforated ulcer. The patient’s best corrected visual acuity (BCVA) was reduced to hand motion in the left eye and was 20/40 in the right eye, with the intraocular pressure within the normal range in both eyes. The patient was previously diagnosed with fungal keratitis following trauma but was non-compliant with topical antifungal agents and did not maintain a proper follow-up. A sclerokeratoplasty using a 14 mm corneal graft, as well as iridectomy and lensectomy, was performed in her left eye. The corneal graft remained clear at 4-week follow-up, and her BCVA improved to 20/100 after aphakic correction (figure 1B).

{kind=link}
(A) The lesion had a typical blueberry-like external appearance, consisting of an extremely thin and protruded cornea, measuring 12×14 mm, with iridocorneal adhesions. (B) The patient underwent sclerokeratoplasty using a 14 mm corneal graft, as well as iridectomy and lensectomy. The graft remained clear at 4-week follow-up, and the patient’s best corrected visual acuity improved to 20/100 after aphakic correction.
The patient was diagnosed with acquired total anterior staphyloma, a rare anterior segment pathology that occurs due to protrusion of uveal tissue through a prominent defect in the cornea or sclera, as a consequence of trauma, corneal ulcers, vitamin A deficiency, or congenitally as component of Peters anomaly.1 Typically the incidence of acquired anterior staphyloma is seen in low-income/middle-income countries as a result of non-availability of proper care post trauma, in cases of infectious keratitis or due to poor patient compliance to treatment.2
Learning points
Patients at a high risk of ocular surface infections post trauma should be encouraged for a regular follow-up at short intervals of time.
The attending ophthalmologist should ensure compliance of the prescribed regimen of drugs to prevent deterioration of infective keratitis.
A surgical intervention, if required, should be performed at an early stage to salvage as much ocular surface tissue as possible and prevent complications such as staphyloma.
Footnotes
Contributors RBS and ST diagnosed the case. RBS and KPS wrote the manuscript. ST was actively involved in the patient’s surgical management.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.