Article Text

Statistics from Altmetric.com
Description
An 87-year-old man with history of dementia, coronary artery disease on dual antiplatelet therapy and oesophagitis presented to the emergency department with acute-onset coffee ground emesis and left upper quadrant abdominal pain of 1-day duration. Vital signs were normal. Exam was notable for diffuse abdominal pain without peritoneal signs.
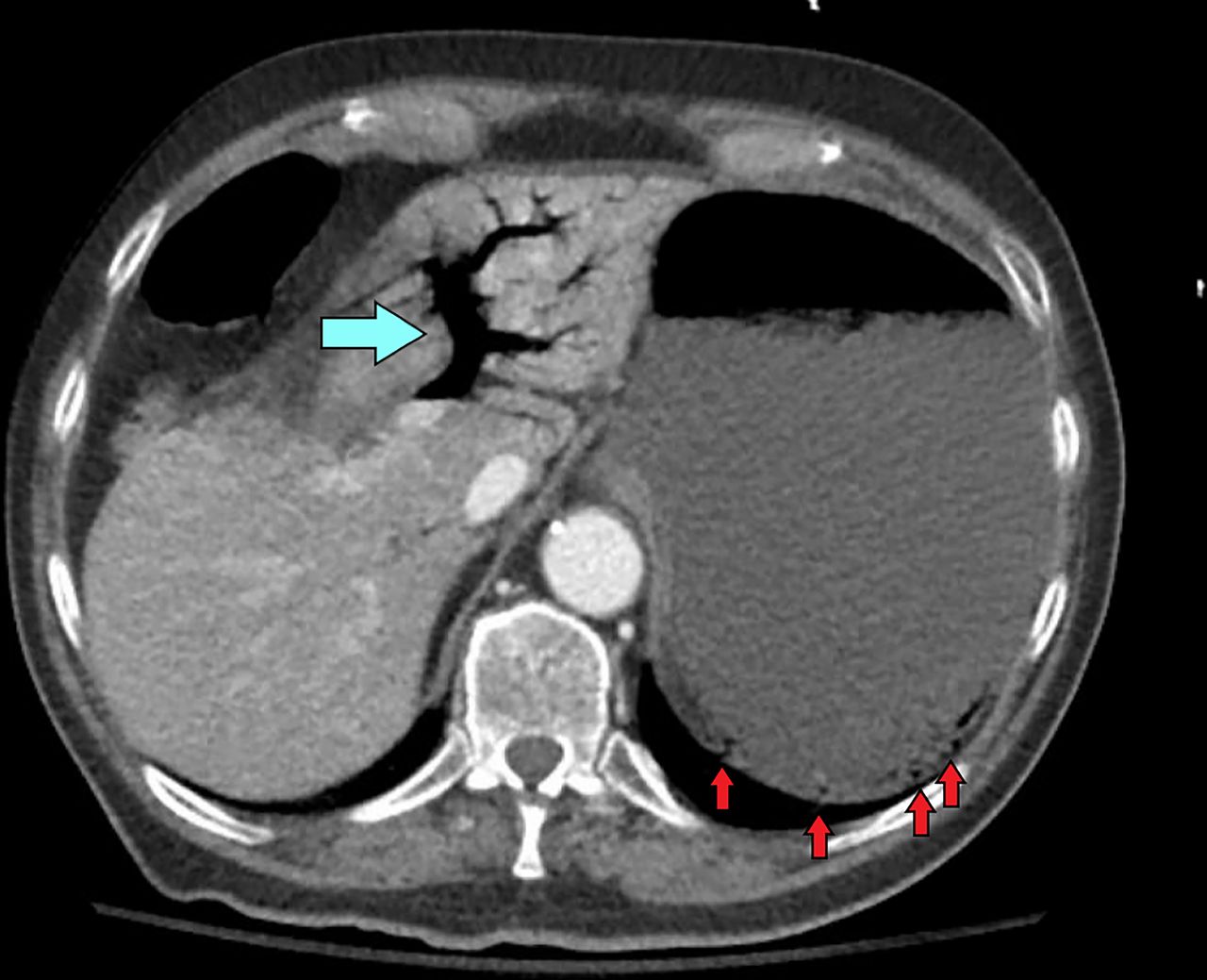
Medical work-up was remarkable for haemoglobin of 8.2 g/dL, lactate of 6.3 mmol/L and white blood cell count of 21.84x109/L. CT with angiography of the abdomen and pelvis revealed extensive portal and mesenteric venous gas as well as gastric emphysema (figures 1 and 2). The bowel was normal.

Axial CT image of the upper abdomen with intravenous contrast demonstrates extensive portal venous gas (blue arrow). Multiple locules of gas (red arrows) are present in the wall of the stomach.

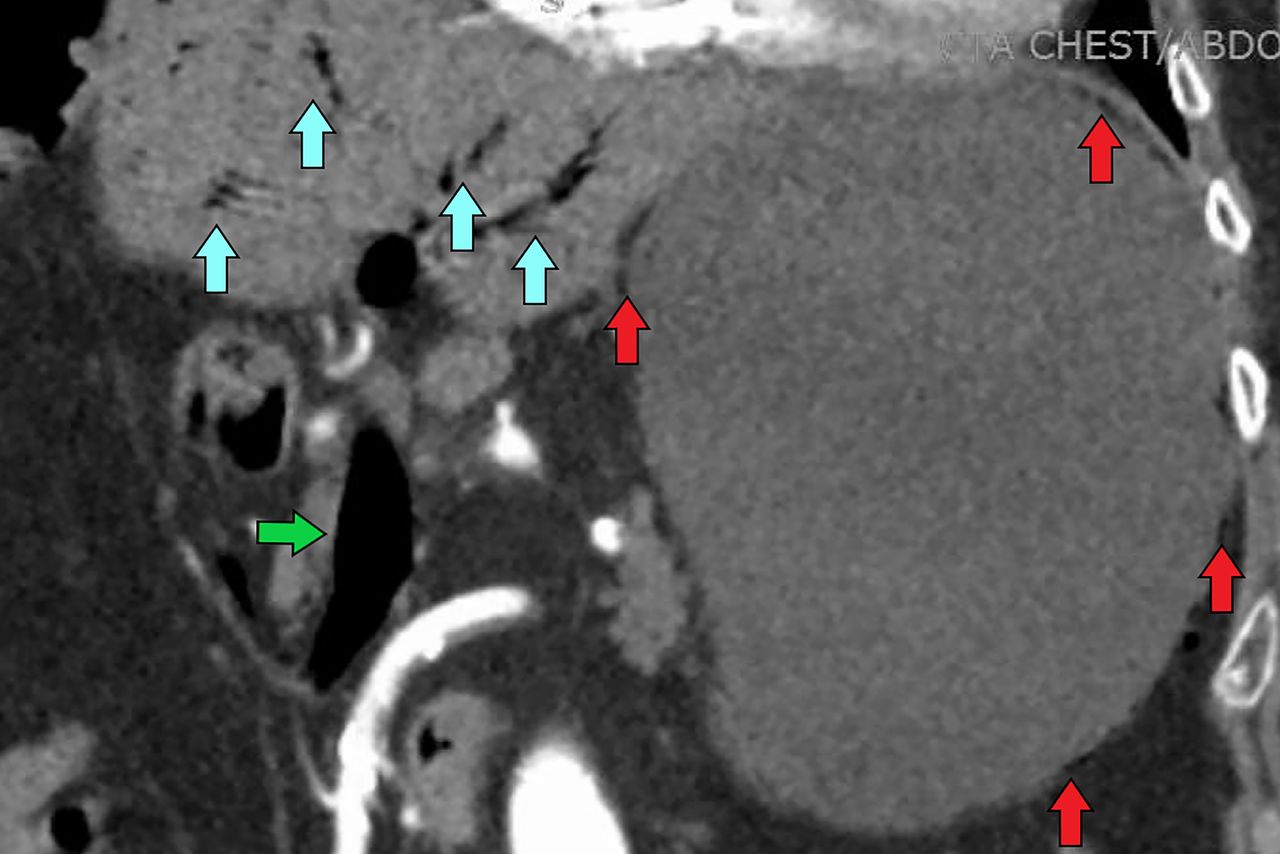
Coronal CT of the upper abdomen with intravenous contrast demonstrates extensive portal venous gas (blue arrows). Gas is also present in the superior mesenteric vein (green arrow). Multiple locules of gas (red arrows) are present in the wall of the stomach.
Exploratory laparotomy was performed to evaluate for bowel ischaemia. It demonstrated normal bowel, while upper endoscopy demonstrated diffuse severe erosive and necrotic gastritis (figure 3), consistent with emphysematous gastritis. In addition to fluids and a proton pump inhibitor, antibiotics were initiated for suspected infectious aetiology. Blood cultures were negative. Gastric biopsy findings were consistent with acute phlegmonous gastritis secondary to Sarcina ventriculi, a rare organism implicated in severe gastric pathology, with predisposition towards patients with delayed gastric emptying (not in our patient though). Within 24 hours, repeat non-contrast CT of the abdomen and pelvis demonstrated resolution of portal venous gas and gastric emphysema (figure 4), with resolution of patient symptoms. A repeat endoscopy 5 days later revealed resolution of necrosis without ulceration.

Upper endoscopy image of the stomach demonstrates diffuse inflammation and necrosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Axial CT image of the upper abdomen without intravenous contrast at 24 hours post-treatment with antibiotics demonstrates resolution of portal venous gas. The stomach wall is diffusely thickened with resolution of air in the wall.
Emphysematous gastritis is a rare, life-threatening form of gastric emphysema due to gas-forming bacteria, where clinical presentation in combination with imaging is crucial for accurate diagnosis.1–3 Notably, gastric emphysema is a benign finding and may look identical on imaging. Essential diagnostic features of emphysematous gastritis include severe abdominal pain, haematemesis and high lactate, whereas patients are generally asymptomatic with gastric emphysema. Early recognition is important to allow for immediate initiation of broad-spectrum antibiotics and fluid support.2 Surgery is indicated if gastric infarction is suspected via endoscopy.1
Learning points
Emphysematous gastritis is a life-threatening form of gastric emphysema.
Diagnosis is based on a combination of imaging, clinical and endoscopic findings.
Urgent identification and initiation of antibiotics are essential, although mortality rates remain high despite treatment.
Footnotes
Contributors NAJ provided both the initial diagnosis and care of the patient, respectively. MA wrote the initial manuscript, which was subsequently reviewed and edited by NAJ.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.