Article Text

Statistics from Altmetric.com
Description
A 60-year-old, previously healthy woman presented with patchy skin colour change and dryness for 3 months duration. She also gave a history of recurrent boils requiring local and oral antibiotics. On examination, patchy hyperpigmented skin with scaly appearance was apparent along with features of healed and active infection (figure 1). She also had multiple, firm, lymph nodes (largest 2 cm) in the bilateral axillae. On evaluation, haemoglobin was 115 g/L, white blood cells 7.8×109/L, platelets 248×109/L; peripheral blood smear was normal. Representative skin biopsy showed loss of granular layer characteristic of ichthyosis (figure 2). Right axillary lymph node excision biopsy and immunohistochemistry confirmed the diagnosis of T-cell non-Hodgkin’s lymphoma (not otherwise specified). HIV ELISA, thyroid function tests and coeliac serology were inconclusive. She was treated with cyclophosphamide, doxorubicin, vincristine and prednisolone chemotherapy along with moisturisers (urea-based), regular skin cleansing and salty water bath. After six cycles of chemotherapy, she achieved complete remission with partial improvement in ichthyosis.
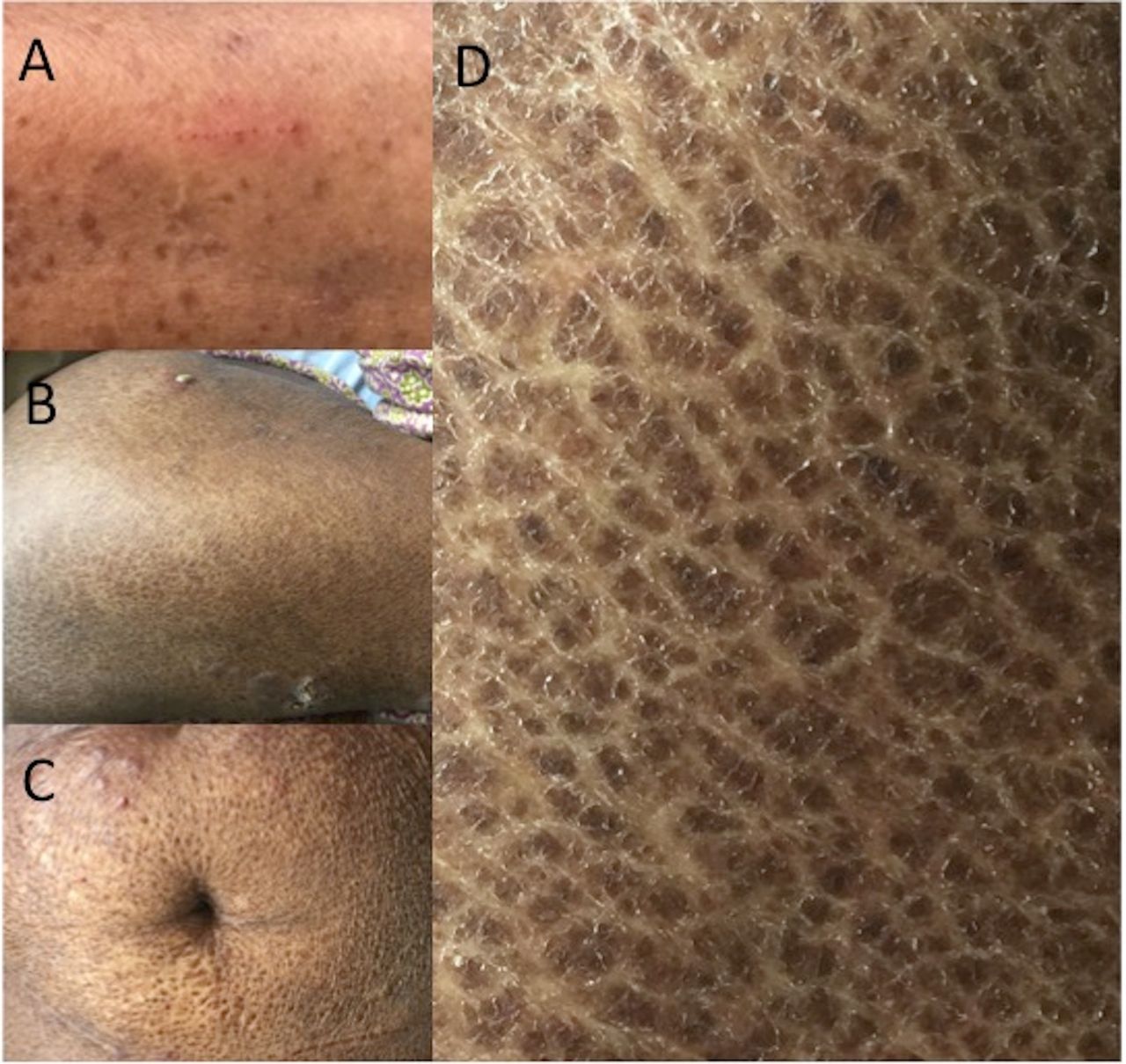
(A) Clinical photograph showing scaly, hyperpigmented lesions over upper limb with a linear lesion resulting from scratching; (B) ichthyosis and associated healed lesions over lower limb along with a pustule; (C) ichthyosis along with healed lesions over abdomen; (D) typical hyperpigmented scaly lesions over back giving rise to ‘fish scale’ appearance.

{kind=link}
{kind=link}
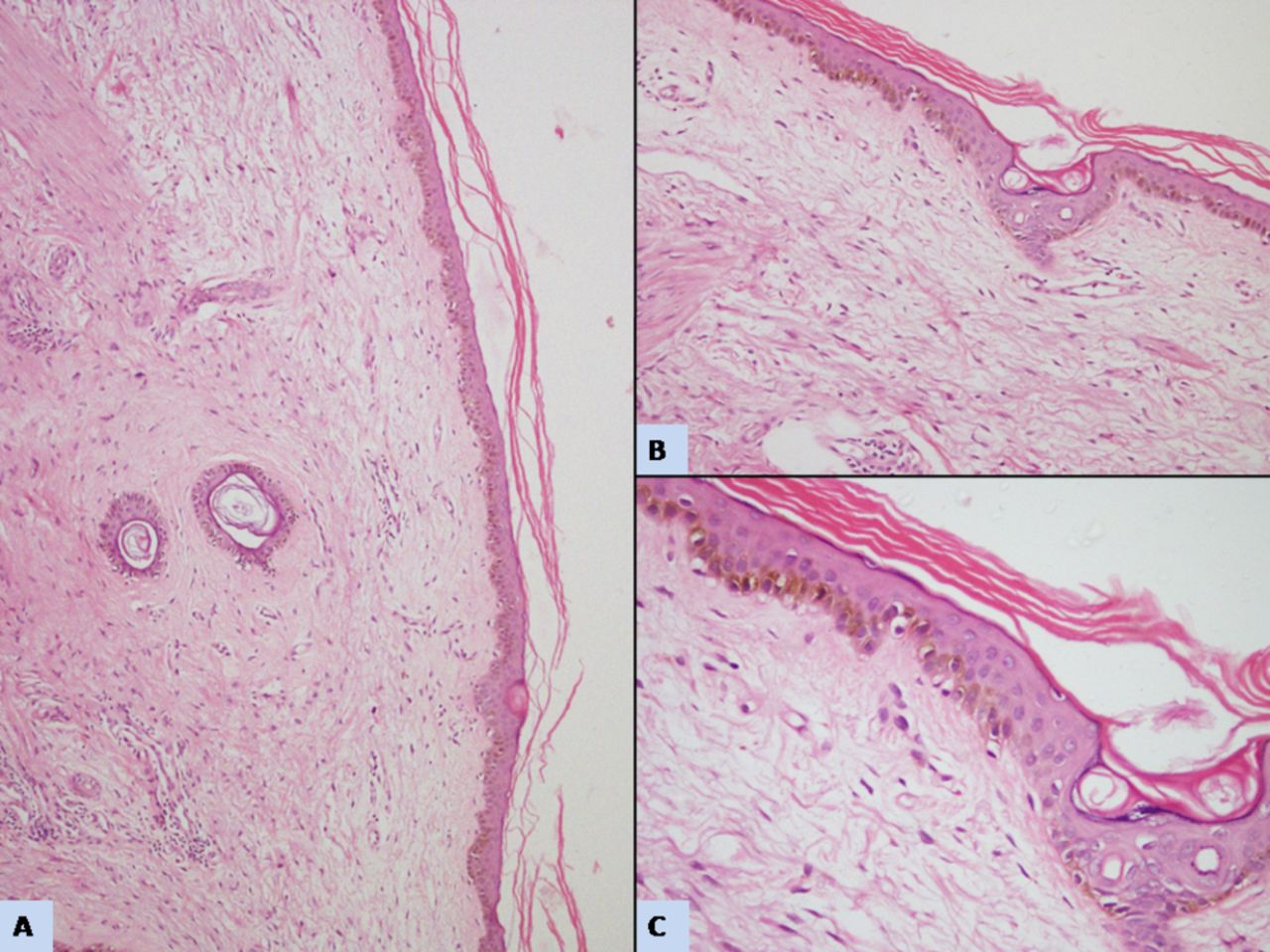
(A) Low magnification of skin biopsy showing epidermis and dermis (H&E ×100); (B) epidermis demonstrates loss of normal basket weave pattern (H&E ×200); (C) high magnification demonstrates loss of granular layer within the epidermis, characteristic of ichthyosis (H&E ×400).
Acquired ichthyosis is an uncommon dermatosis characterised by disrupted skin cornification. Herein, dry and thickened skin confers the characteristic ‘fish-like’ appearance and significant morbidity in the form of itching, heat intolerance, recurrent infections and restricted joint mobility. Besides neoplastic disorders (Hodgkin’s lymphoma, anaplastic large cell lymphoma, mycosis fungoides, POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal protein, skin changes) syndrome, etc), it is known to be associated with malnutrition, infections (HIV, Human T-lymphotropic virus (HTLV)), hypothyroidism, coeliac disease, sarcoidosis, graft-versus-host disease and drug intake (hydroxyurea, allopurinol, vemurafenib, etc).1 2 Hence, it is crucial to emphasise that new-onset ichthyosis in any adult patient should be actively evaluated to unveil the underlying cause. Management consists of treatment of the underlying cause together with measures directed at reducing skin dryness and scaling.3 T-cell non-Hodgkin’s lymphoma (NOS) presenting with ichthyosis has rarely been described in literature; probably due to short survival. In the index case, occurrence of unapparent additional factors (eg, nutritional deficiency, autoimmune disorder, etc) shall explain incomplete resolution of ichthyosis.
Learning points
Footnotes
Contributors All authors contributed to the management of the patient. KM and AJ prepared the manuscript, which was read and accepted by all the authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.