Article Text

Statistics from Altmetric.com
Description
Intramural duodenal haematoma (IDH) is a rare condition forming haematoma within the wall of the duodenum, which was first reported in 1838 by MacLauchlan.1 IDH derived from acute or chronic pancreatitis is rarely described, the mechanism remaining unknown. A 65-year-old man with history of heavy drinking and chronic hepatitis was admitted to our hospital with sudden vomiting and right-lateral abdominal pain. Abdominal pain and vomiting continued after admission, so a nasogastric tube was inserted. Contrast-enhanced CT scans of the abdomen found a 60×80 mm heterogeneous mass with intraluminal leakage of contrast agent-like bleeding along the second portion of the duodenum, diffuse expansion of the pancreatic duct with pancreatic stone and ascites on the surface of the liver (figure 1). We first considered whether the mass might be duodenal gastrointestinal stromal tumour with internal bleeding according to symptoms and enhanced CT image. However, gastrointestinal endoscopy showed mucosal redness and protrusion into the lumen at the second portion of the duodenum, which was flattened when air was delivered. Additionally, endoscopic ultrasound and MRI found that the mass contained only fluid without solid component. We finally diagnosed IDH according to these examinations. IDH often improves with conservative treatment.2 The indication for conservative treatment of IDH is to satisfy the following; no other organ damage, no major bleeding, and improvement of obstructive symptoms by 7–10 days after the start of treatment. Although our patient also was treated conservatively with fasting and infusion therapy for 2 weeks, he continued bleeding and duodenal obstruction. So we performed percutaneous drainage to reduce haematoma. Initially, drainage discharge was bloody, but turned clear on day 2. Biochemical examination of drainage discharge showed high amylase levels of more than 100 000 (U/L). From percutaneous drainage tube, 100–150 mL/day of clear fluid continued to be discharged, so we suspected there was fistula between IDH and the pancreatic duct. Contrasting from a percutaneous drainage tube placed in IDH exhibited the caudal pancreatic duct and proved the presence of fistula (figure 2). From these results, it was found that the pancreatic fistula due to exacerbation of chronic pancreatitis contributed to the formation of IDH. Endoscopic treatment was considered the first choice, but in this case Frey procedure was performed because there was also the influence of chronic pancreatitis accompanied by many huge pancreatic stones.3 After transecting the pancreatic duct, we collected many pancreatic stones and performed pancreaticojejunal anastomosis and jejunojejunostomy for the Roux limb. Discharge of pancreatic juice from the percutaneous drainage tube decreased remarkably after surgery. On postoperative day 12, percutaneous drainage tube could be withdrawn. The mechanism of IDH associated with pancreatitis has never been reported and this case is the first.

Enhanced CT images of the abdomen show large mass lesion with the intraluminal leakage of contrast agent along the second portion of the duodenum. They also reveal diffuse expansion of pancreatic duct, huge pancreatic stone (black arrow) and ascites on the surface of the liver (A–C).
{kind=link}
{kind=link}
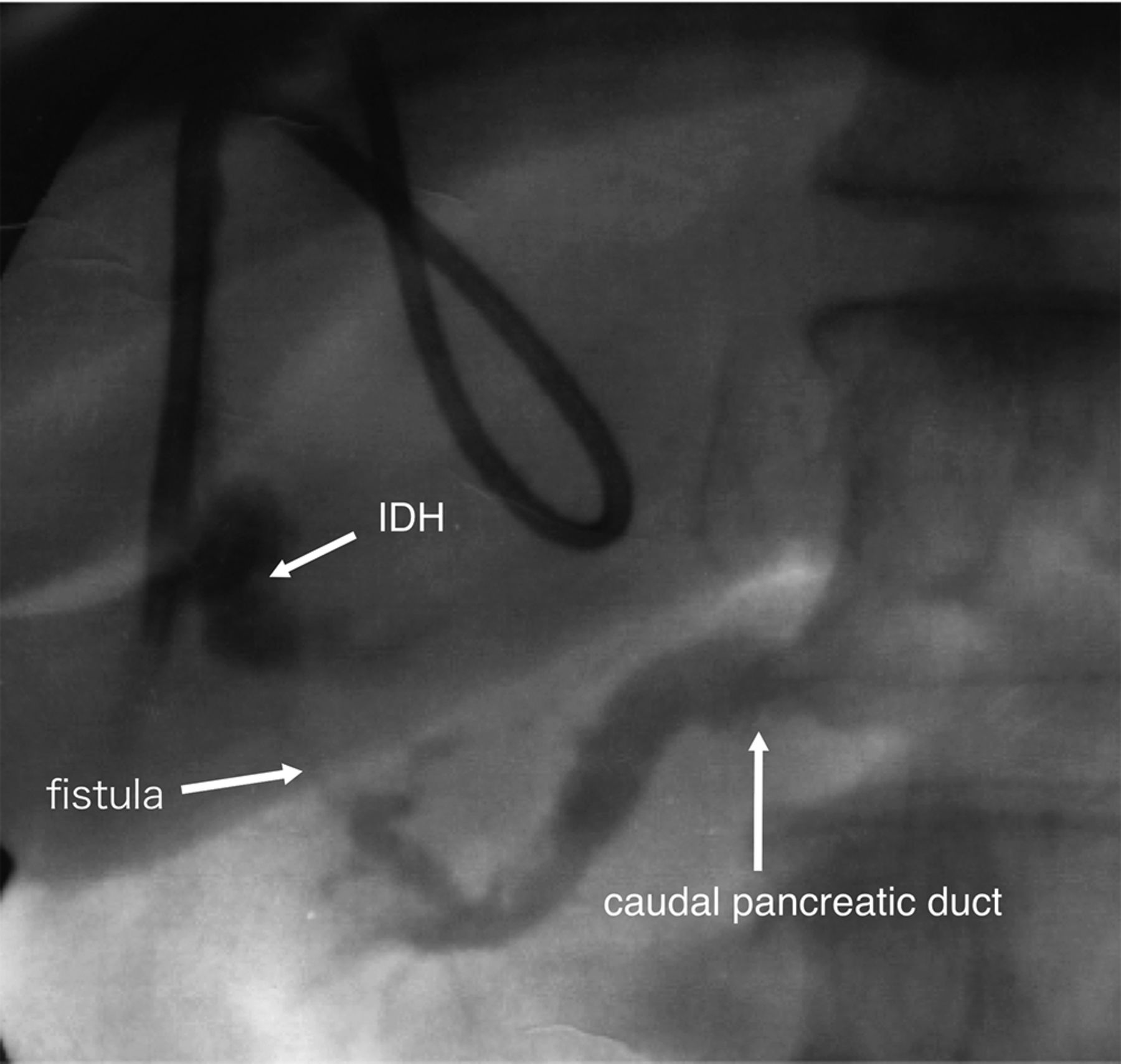
Contrasting from a percutaneous drainage tube in the intramural duodenal haematoma (IDH) shows the fistula from the pancreatic duct.
Learning points
Intramural duodenal haematoma (IDH) has often been described as a complication of blunt trauma to the abdomen and iatrogenic trauma, and IDH derived from acute or chronic pancreatitis is rarely described.
A pancreatic fistula due to pancreatitis contributed to the formation of IDH in this case.
Footnotes
Contributors JK is the first author and corresponding author of this manuscript. HN collected the clinical data. NY and KS revised the manuscript. All authors read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.