Article Text

Statistics from Altmetric.com
Description
A 29-year-old never-smoking woman who had been diagnosed with Marfan syndrome at 9 years of age was admitted with persistent exertional dyspnoea. She had previously developed pneumothorax three times and underwent scoliosis surgery and aortic valve replacement. A physical examination revealed a thin, healthy-appearing woman (body mass index 16.4 kg/m2) with pectus excavatum and joint hyperflexibility.
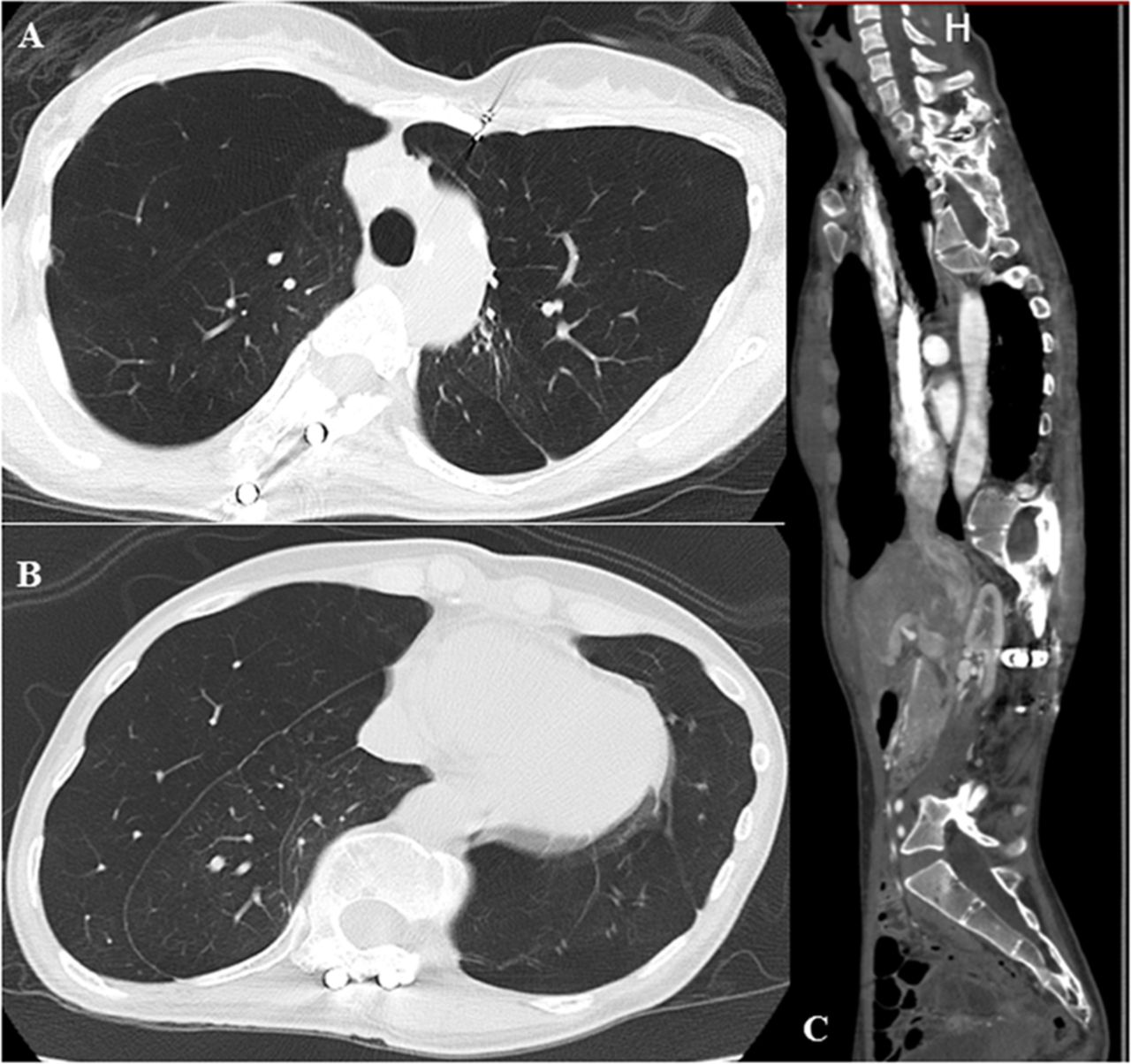
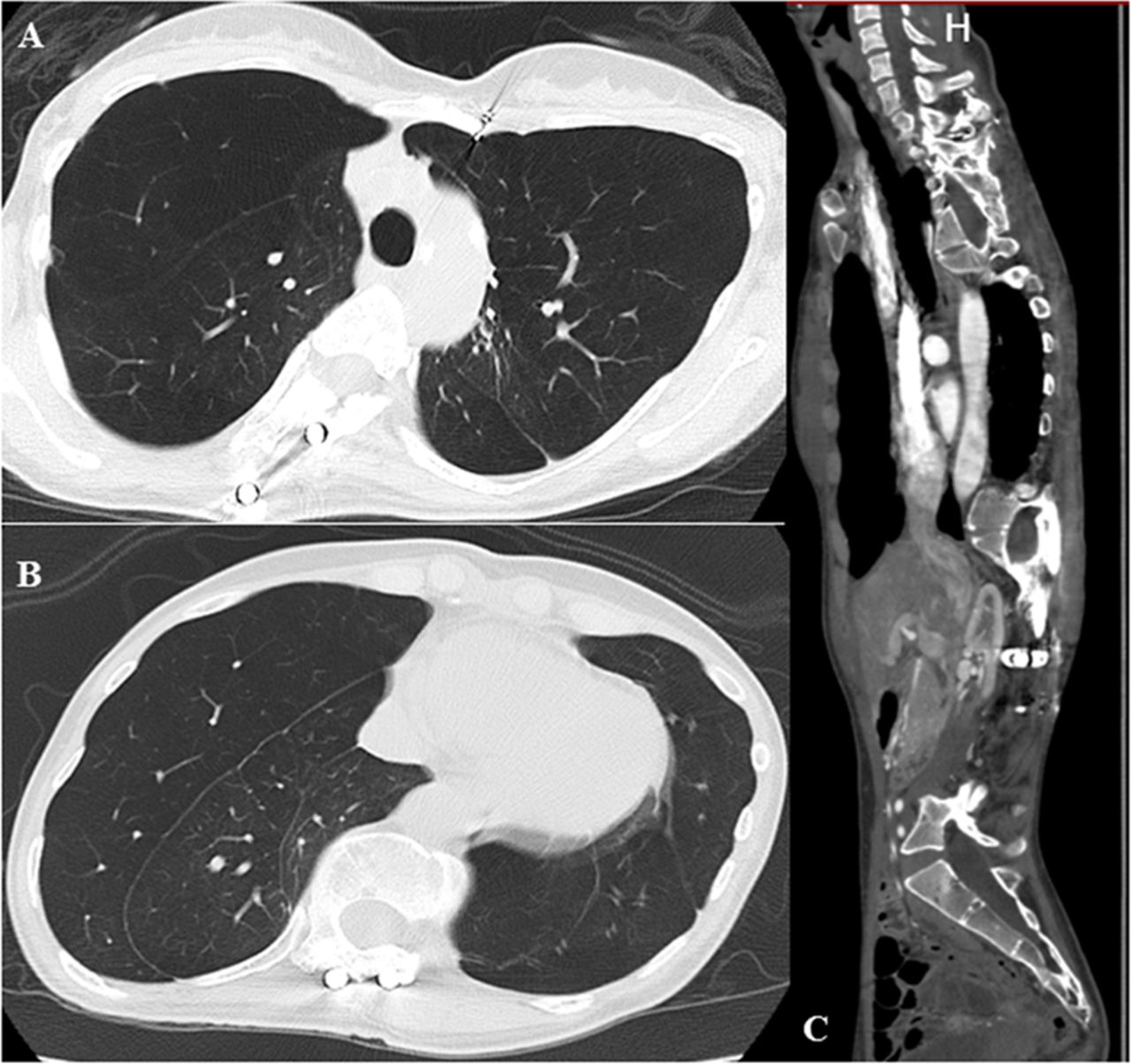
Chest radiography (figure 1) and CT (figure 2) showed severe spinal deformity and diffuse emphysematous change of the lungs. Pulmonary function tests showed a forced vital capacity of 2.7 L (81% predicted), a forced expiratory volume in 1 s (FEV1) of 1.47 L (49.7% predicted), FEV1% of 53.1% and a diffusing capacity of the lung for carbon monoxide of 48%. The patient has been treated with an inhaled long-acting beta2-adrenergic agonist and long-acting anticholinergic bronchodilator, and her lung function has been maintained at a plateau level for about 8 years.
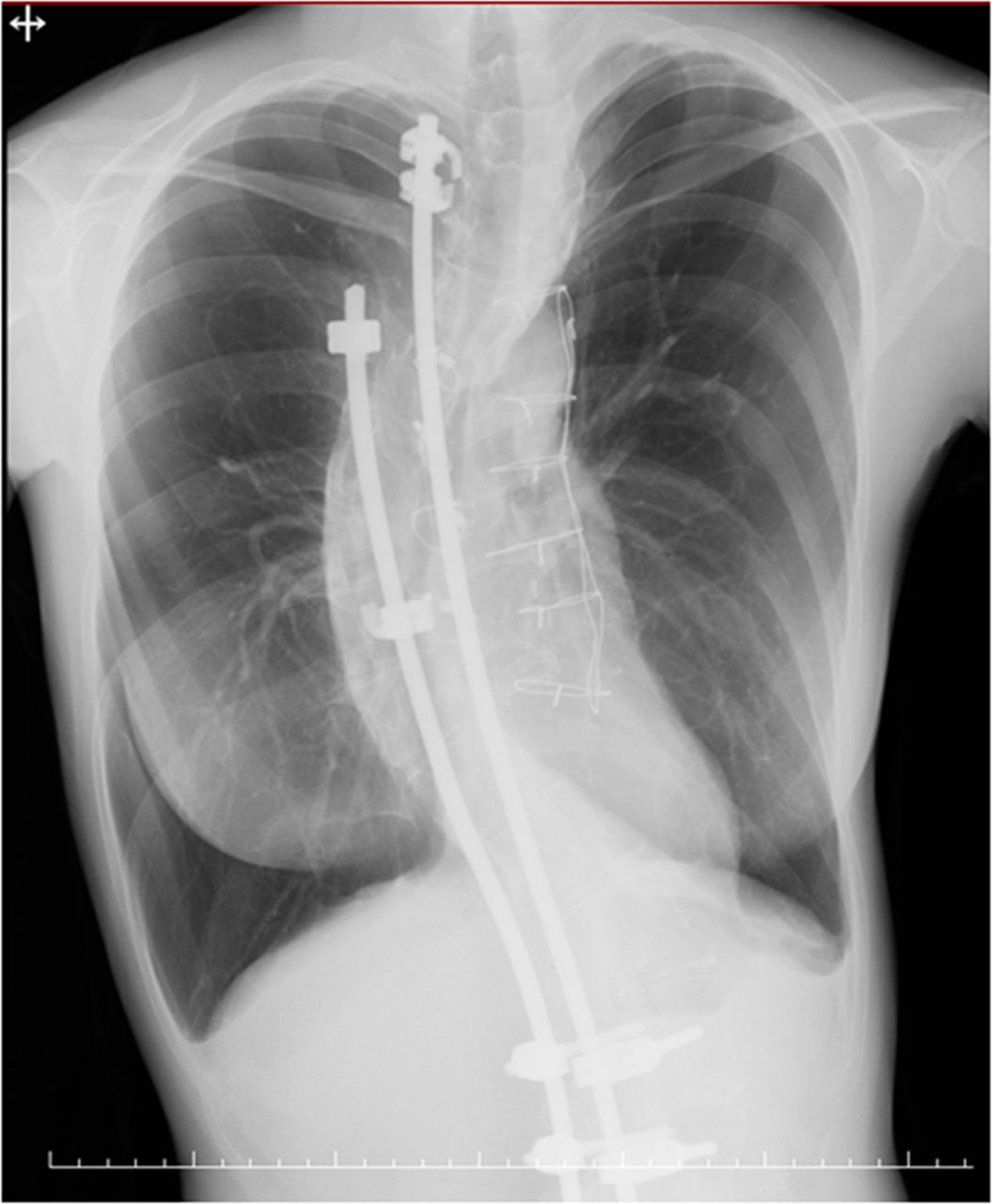
Chest radiography showing spinal deformity and overinflation of the lungs.
{kind=link}
{kind=link}
CT showing severe emphysematous change of the lungs (A, B: axial scanning) and spinal deformity (C: sagittal scanning).
Pulmonary involvement is not generally considered a main feature of Marfan syndrome and there are currently no established screening guidelines for Marfan syndrome-associated pulmonary disease. In addition, reports of patients with Marfan syndrome who present with chronic respiratory symptoms are very rare.1 However, pulmonary function abnormalities are frequently observed in patients with Marfan syndrome, particularly among patients with significant thoracic cage abnormalities.1 Thus far, only a small number of reports have shown cases with pulmonary emphysema, pneumothorax and an obstructive pattern and diffusion impairment on pulmonary function tests.2 3 The present case suggests the importance of careful evaluation and monitoring for Marfan syndrome-associated pulmonary disease.
Learning points
Patients with Marfan syndrome can present with pulmonary emphysema, even if they are never-smokers.
The possibility of coexisting lung disease in patients with Marfan syndrome should be considered, particularly among patients with thoracic cage abnormalities.
Footnotes
Contributors HI researched the topic and wrote the case. RS, YK and HK helped with the research and proofreading of the case report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.