Article Text

Statistics from Altmetric.com
Description
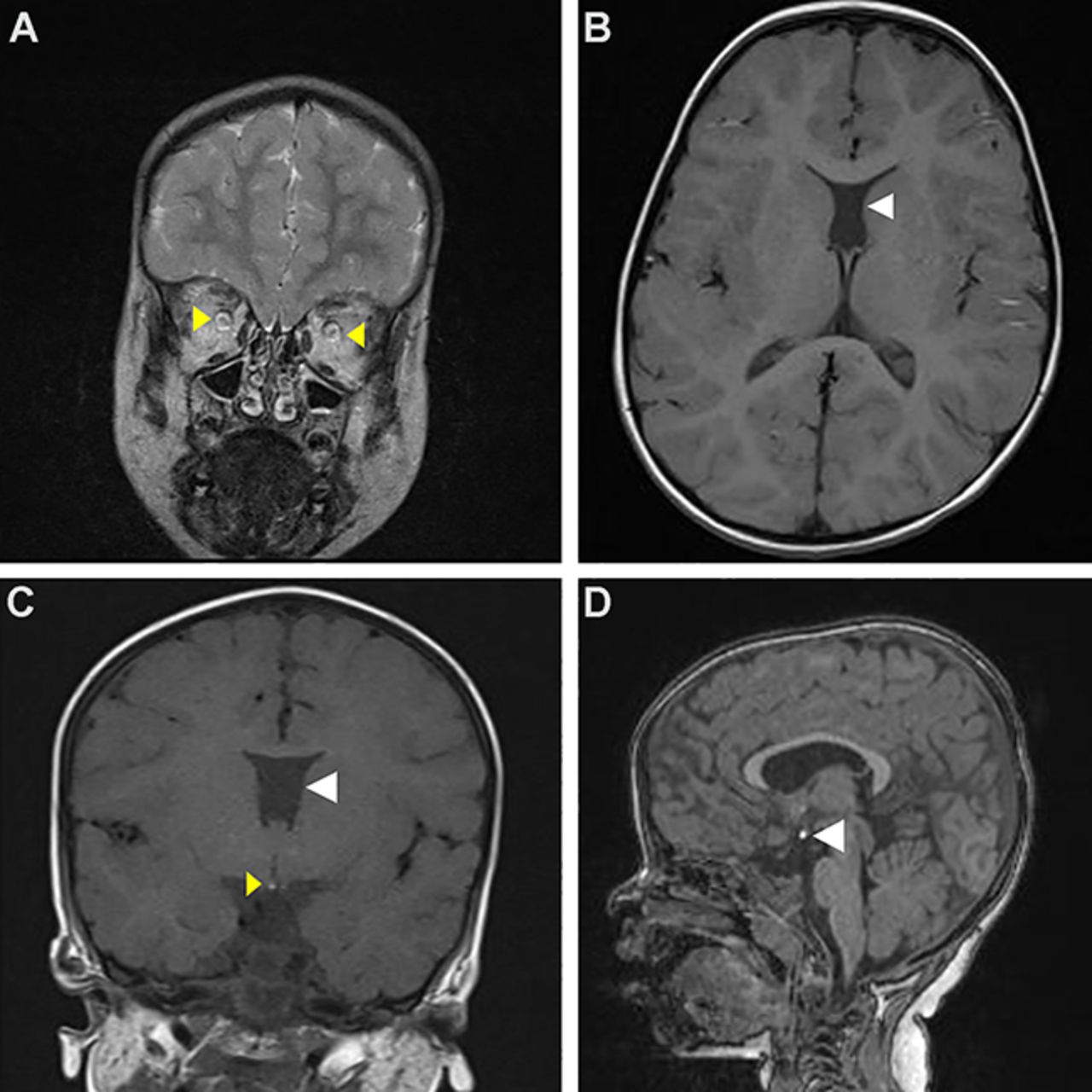
A 3-year-old girl presented to us with short stature, loss of vision in both eyes and strabismus. She had a history of recurrent hypoglycaemia and seizures in the early neonatal period. Ophthalmological examination in infancy revealed bilateral cupping of optic disc and increased intraocular pressure (IOP) for which dorzolamide was started. Later she completely lost her vision, and dorzolamide was discontinued. Clinical evaluation revealed severe short stature and bilateral optic atrophy. Her developmental milestones (both motor and language) were delayed by 1–1.5 years. Her routine blood investigations were normal. Hormonal examination revealed central hypothyroidism, and it was corrected with thyroxine after confirming normal cortisol axis. Her insulin-like growth factor-binding protein 3 was low, and peak growth hormone (GH) level following stimulation was 1.2 µg/L, suggestive of severe GH deficiency. There was no history of polyuria, and serum electrolytes were normal. MRI of the brain revealed bilateral optic nerve hypoplasia (figure 1A), absence of septum pellucidum (Figure 1B; Figure 1C) and ectopic posterior pituitary bright spot (figure 1C,D). Currently, she has gained 4 cm of height in 6 months with GH therapy.

{kind=link}
(A)MRI of brain (T2-weighted coronal view) showing prominent cerebrospinal fluid spaces around optic nerve suggestive of optic nerve hypoplasia (yellow triangles). (B) MRI of brain (T1-weighted axial view) showing absence of septum pellucidum (white triangle). (C) MRI of brain (T1-weighted coronal view) showing absence of septum pellucidum (white triangle) and ectopic posterior pituitary bright spot at the floor of third ventricle (yellow triangle). (D) MRI of brain (T1-weighted sagittal view) showing ectopic posterior pituitary bright spot at the floor of third ventricle (white triangle).
Septo-optic dysplasia (SOD), also known as de Morsier syndrome,1 is a rare congenital anomaly. Two or more features of the triad of optic nerve hypoplasia, pituitary hormone deficiency and midline brain defects (absence of septum pellucidum and/or corpus callosum) are required for the diagnosis of SOD.2 Our patient had all the three components. Rarely, raised IOP can be an associated feature.3
Learning points
Neonatal hypoglycaemia and resultant seizures can be an early clue for diagnosing growth hormone deficiency.
Diagnosis of septo-optic dysplasia requires the presence of two or more features of the triad of optic nerve hypoplasia, pituitary hormone deficiency and midline brain defects.
Clinical evaluation followed by hormonal evaluation and imaging can guide us to its appropriate diagnosis and treatment.
Footnotes
Contributors RP and KS: writing the manuscript and management of the patient. JPS and SK: reviewing the script and management of the patient.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.