Article Text

Statistics from Altmetric.com
Description
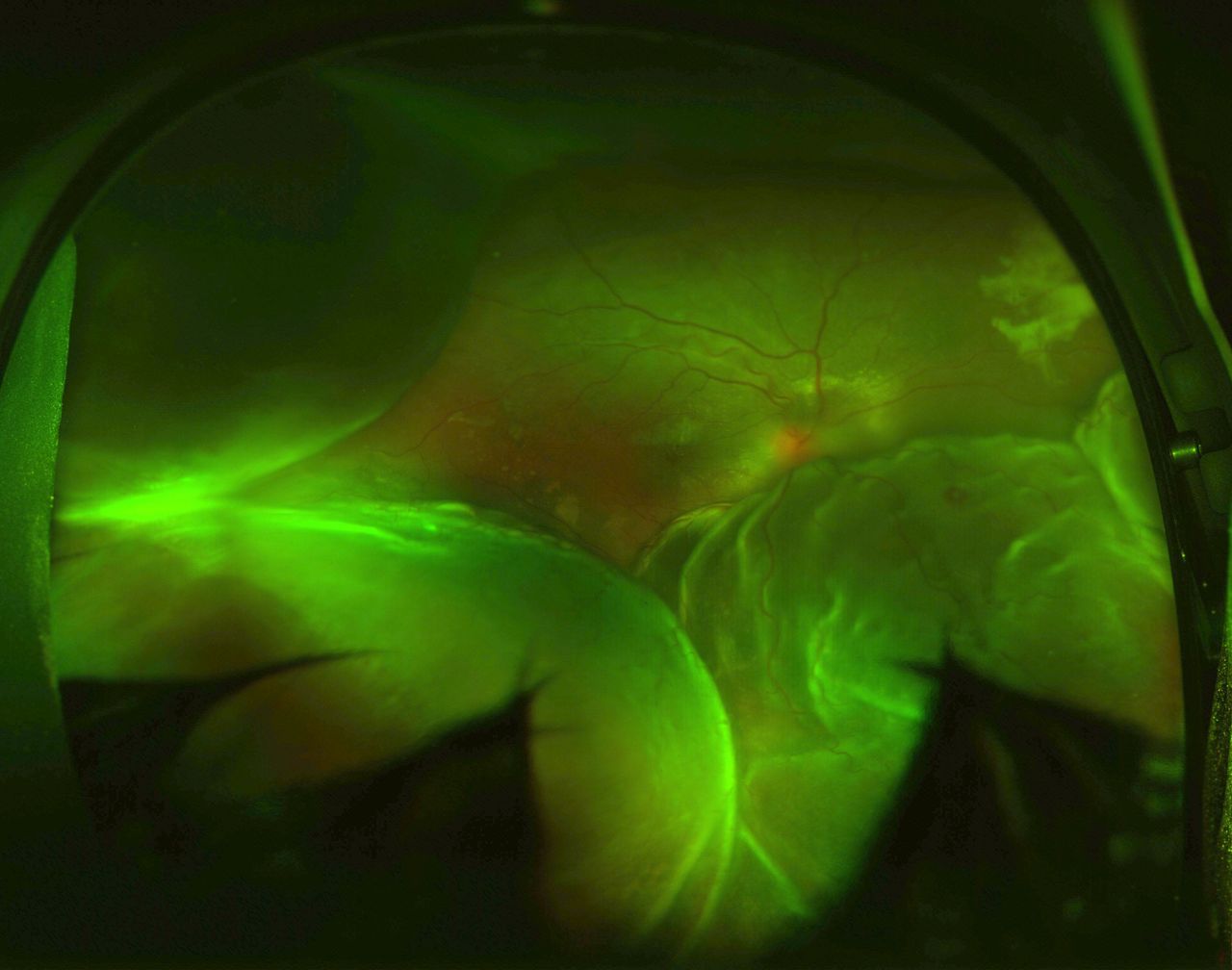
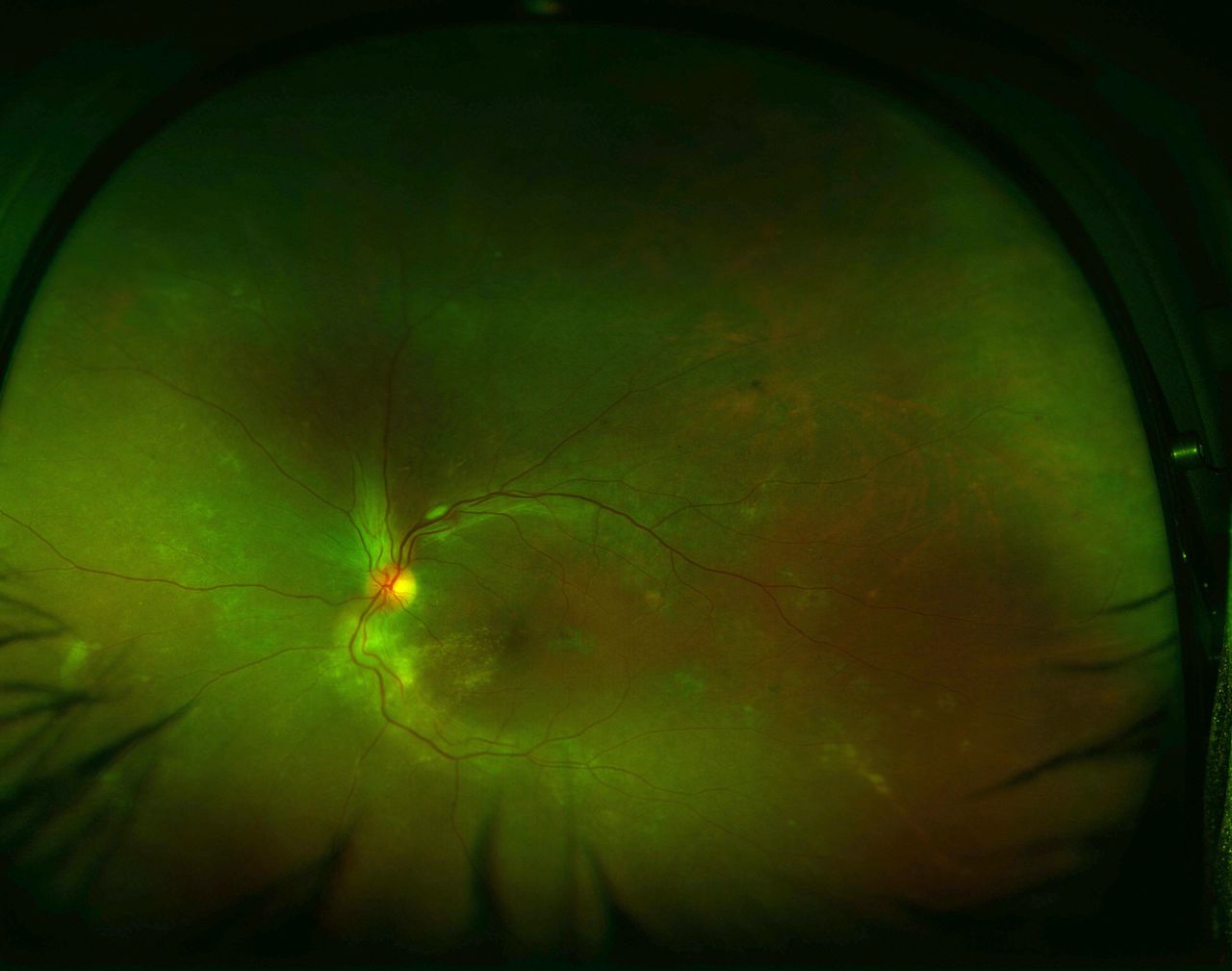
A 35-year-old woman at 26 weeks’ gestation presented with vision loss in the right eye (RE) and abdominal pain for 10 days. There was no fever. RE had conjunctival congestion and chemosis with a visual acuity of finger counting close to face. The RE showed an exudative retinal detachment, disc oedema and choroidal detachment (figure 1). The left eye visual acuity was 6/12 and on examination there was disc oedema, cotton wool spots, subfoveal fluid and Elschnig’s spots (figure 2).1 Ultrasonogram showed echoes beneath the choroidal detachment suggestive of suprachoroidal haemorrhage (figure 3). Intraocular pressure and anterior chamber depth were normal in either eye. The blood pressure (BP) was 200/120 mm Hg. The laboratory investigations included a haemoglobin of 6.7 g/dL (12–15.8 g/dL), platelet count 65x109/L (150x109–300x109/L), total leucocyte count 9.5x109/L (4x109–11x109/L), total protein 4.8 g/dL (6.7–8.6 g/dL), serum glutamic-oxaloacetic transaminase 29 U/L (12–38 U/L), serum glutamic-pyruvic transaminase 13 U/L (7–41 U/L), urea 108 mg/dL (15–40 mg/dL) and creatinine 6.8 mg/dL (0.6–1.2 mg/dL). Abdominal ultrasound revealed intrauterine fetal death and a gallbladder stone. The patient needed intravenous labetalol, nitroglycerine and oral antihypertensives for control of BP. Systemic management included haemodialysis, blood transfusions, intravenous antibiotics and medical termination of pregnancy, following which the medical condition was stabilised. At 2 months’ follow-up, the patient had a vitreous haemorrhage (vision RE - hand movements close to face) in RE but the ocular ultrasound did not show any choroidal or retinal detachment. The left eye had recovered to 6/6. The patient was lost to follow-up.

The ultrawide fundus image shows disc oedema, mounds of choroidal detachment and an inferior bullous exudative retinal detachment in the right eye.

The left eye showed papilledema, cotton wool spot superotemporal to the optic disc, hard exudates inferotemporal to the optic disc and Elschnig’s spots in the temporal retina.

{kind=link}
{kind=link}
{kind=link}
Ultrasound B-scan of the right eye revealed mounds of choroidal detachment with echoes beneath the mounds suggestive of suprachoroidal haemorrhage.
Spontaneous suprachoroidal haemorrhage (SSCH) is a rare entity and has been known to be associated with anticoagulation therapies (including warfarin, aspirin, clopidogrel, heparin), thrombolytic drugs (streptokinase, tissue plasminogen activator), blood dyscrasias, haemodialysis and Valsalva manoeuvre.2 Systemic predispositions include hypertension, atherosclerosis, cerebrovascular attack, coronary artery disease, diabetes mellitus, chronic renal failure, hepatic failure and disseminated intravascular coagulation.2 Ocular associations are age-related macular degeneration, glaucoma, high myopia and proliferative diabetic retinopathy.2 Hypertension alone has been reported to cause SSCH with secondary angle closure glaucoma.3 Risk factors for SSCH and exudative retinal detachment in our case include pregnancy-induced hypertension (PIH), anaemia, thrombocytopenia, hypoproteinaemia and renal failure. However, control of systemic risk factors resulted in the resolution of the exudative retinal detachment and SSCH. No surgical intervention was planned in view of normal intraocular pressure, the absence of kissing choroidals and deranged systemic status. To the best of our knowledge, an association of SSCH with PIH has not been reported before.
Learning points
Spontaneous suprachoroidal haemorrhage may occur in pre-eclampsia/eclampsia with thrombocytopenia.
Control of systemic parameters is of paramount importance in the management of such a disease.
Footnotes
Contributors KT, VM and HS collected the data. KT and RC wrote the first draft. All authors revised the draft with important intellectual content and approved the final version. All authors agree to be accountable for the work.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.