Article Text

Summary
This report describes a 63-year-old generally healthy male with septic olecranon bursitis caused by Propionibacterium acnes. The patient sustained a small laceration after striking the posterior aspect of his left elbow on a metal railing when he was at a public swimming pool. We concluded that P. acnes was not initially detected because cultures were only kept for 5 days. Consequently, initial antibiotic treatment failed. P. acnes and Staphylococcus epidermidis grew in a subsequent tissue culture. The infection did not respond to intravenous vancomycin although soft-tissue debridements were done. This likely reflected the presence of olecranon osteomyelitis (seen on MRI scans) in addition to inadequate treatment with this antibiotic in the setting of a polymicrobial infection. Eventually, the infection was eradicated with multiple soft-tissue debridements in addition to the continuation of vancomycin with daily intravenous piperacillin/tazobactam that was added for the final 4 weeks of antibiotic treatment.
- bone and joint infections
- orthopaedics
- orthopaedic and trauma surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
The olecranon bursa is thought to be at increased risk for infection due to its superficial location. Septic olecranon bursitis is most commonly caused by bacterial infection with Staphylococcus aureus.1 Ho et al2 found S. aureus to be the predominant cause of infection in 72%–92% of cases that they studied.
Here we report a unique case of a 63-year-old man who sustained a punctate laceration on the posterior aspect of his left elbow and acquired a rare polymicrobial infection (Propionibacterium acnes and Staphylococcus epidermidis) in his olecranon bursa. There was also the possibility of concurrent olecranon osteomyelitis as seen on MRI. The infection was treated successfully with intravenous antibiotics and soft-tissue debridements.
Case presentation
In February 2015, a 63-year-old man (height: 178 cm; weight: 82 kg; body mass index: 26) sustained a punctate laceration on the posterior aspect of his left elbow. At that time he was otherwise healthy and was not taking any medications. He had a medical history of poliomyelitis as an adolescent with mild residual elbow contractures as a result. He was an avid swimmer and swam for exercise three to four times each week at a public pool. He noticed the left elbow laceration after striking the posterior aspect of his left elbow on a metal railing while swimming in a public pool. Two days later erythema and oedema developed around the wound. Five days later he saw his primary care physician who diagnosed this as cellulitis with infected olecranon bursitis. The bursa was lanced to allow it to drain and one culture was obtained from the scant fluid.
The initial culture showed no growth on anaerobic media but it was held for only 5 days, which is not sufficient for detecting P. acnes; growth of this organism usually requires 9–14 days.3 The patient’s primary care physician prescribed a 5-day course of intramuscular injections of ceftriaxone 1.0 g daily and a 10-day course of doxycycline 100 mg orally two times per day. The rationale given for its combination was ‘for broad antibacterial coverage’.
The patient was referred to our clinic to take over the management of his septic left olecranon bursitis because of the clear failure of his initial treatment regimen. At that time, he was applying small gauze dressings two times per day to cover and collect the drainage from the 1-centimetre diameter open wound over the olecranon. MR images of the left elbow suggested mild acute osteomyelitis of the olecranon. At this clinic visit, one culture of the tissue that was cut with a scalpel from the open wound of the left olecranon bursa was obtained. The methodology for the anaerobic culture included cooked meat glucose liquid broth, plating on anaerobic blood agar and anaerobic blood agar containing phenyl ethyl alcohol which selects for Gram-positive organisms. P. acnes grew only in cooked meat glucose liquid broth under anaerobic conditions with no colonies observed on solid medium. Cultures were kept for 14 days. P. acnes was identified by MALDI TOF mass spectrometry. Analysis for P. acnes phylotypes was not done although this information can be clinically important in some situations. S. epidermidis was also detected from the same culture when plated on aerobic blood agar. Antibiotic sensitivities were not done on either organism, which was an error because the laboratory failed to recognise that the sample was bursa tissue.
After obtaining the tissue culture, but prior to receiving the culture results 9 days later, intravenous vancomycin (1.5 g two times per day) had been started by the surgeon. This treatment was continued for 2 weeks. No addition cultures were obtained. Because of continuing drainage and the lack of the expected robust erythematous granulation tissue, ertapenem (1 g once daily) was then added and this two antibiotic treatment was continued for an additional 2 weeks. However, the clinical response to this double antibiotic treatment continued to be poor. Because of this an infectious disease specialist (MRO) was consulted. The consultant stopped ertapenem and started piperacillin/tazobactam 4.5 g intravenously every 8 hours. This change was based on data showing that this penicillin-based antibiotic with a beta-lactamase inhibitor would provide coverage for P. acnes in addition to: (1) continuing broad-spectrum coverage primarily for the possibility that another pathogen (in addition to S. epidermidis) was present but did not grow in subsequent cultures and (2) more aggressively treating the olecranon osteomyelitis.4 5
During the intravenous antibiotic treatments, consecutive weekly irrigation and debridement procedures of the soft tissues were performed in our clinic. These procedures included superficial curettage of the wound base and margins. Two additional soft-tissue irrigation and debridements were done in the operating room. The first of these operating room irrigation and debridements was intended for wound closure. However, the wound was not ready for closure because the granulation tissue was inadequate (figure 1). As described above, this was when piperacillin/tazobactam was added. During the entire course of treatment the bone was never exposed; it was always covered with periosteum/granulation tissue.

Photograph of the patient’s left elbow. The open wound exposes the olecranon bursa region, but the bone was never exposed during the entire course of treatment.
After piperacillin/tazobactam was started, the wound started to granulate well and was closed after 18 days of treatment with this antibiotic. Closure included a Z-plasty and retention stitches with bolsters which enabled closure of the retracted skin margins (figure 2). After closure, the patient’s left upper extremity was placed in long-arm cylinder cast at 30° of elbow flexion. The cast was changed every 2 weeks and the elbow flexion angle was increased 30° each time. This regimen was done to allow wound healing without excessive skin tension. The wound healed uneventfully (figure 3).

Photograph of the patient’s left elbow showing the lesion closed with retention stitches. The stitches are passed through 0.5 cm segments that were cut from a narrow rubber tube, which are bolsters that serve to distribute stress so that the stitches do not cut through the skin.

Photograph taken 4 months after the elbow wound was closed. The wound had healed well and without any problems at final follow-up, which was 14 months after this photograph was taken.
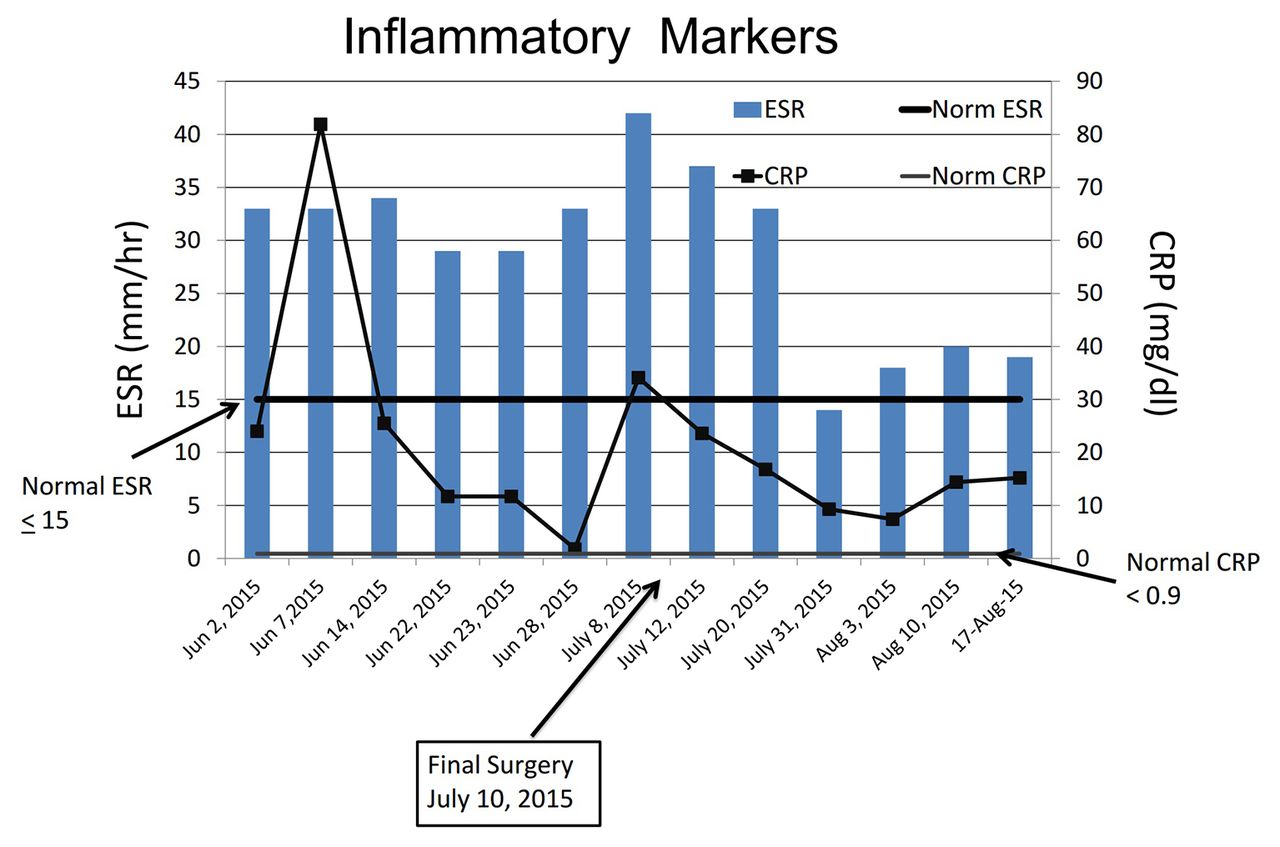
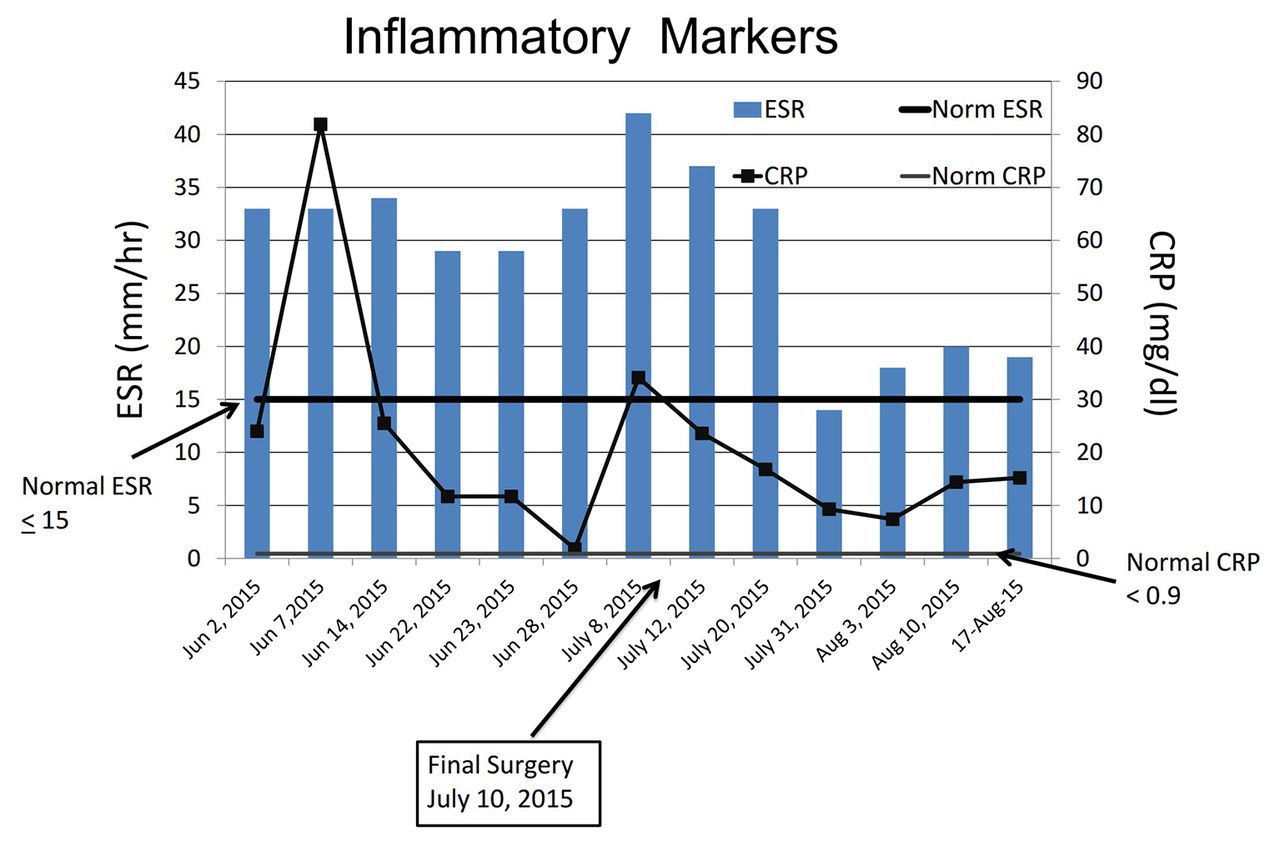
The patient’s C reactive protein (CRP) and erythrocyte sedimentation rate (ESR) results are shown in figure 4. These values were never within normal limits during the course of treatment, which we attributed to inflammation associated with osteoarthritis of his elbows.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The patient’s erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) values throughout his course of treatment.
Outcome and follow-up
Final follow-up was at 30 months after the final wound closure. The patient had resumed his work in manual labour, had no complaints and remained free of infection.
Discussion
To our knowledge this is the first reported case of infected olecranon bursitis with the causal organisms being S. epidermidis and P. acnes, as shown in cultures from a tissue specimen. The association with P. acnes is the most unusual aspect of this case. Despite the shortcomings of the initial aspects of treatment for this case, including the initial courses of inadequate antibiotic treatments (eg, the primary care physician’s use of low dose ceftriaxone and the surgeon’s use of vancomycin instead of a beta-lactam antibiotic for P. acnes), this case is reported in order to help other medical doctors and surgeons avoid these pitfalls. Additionally, at the time when these decisions were made our literature searches (PubMed and Google) of ‘P. acnes’ and ‘olecranon’ and ‘olecranon bursitis’ failed to reveal any cases.
P. acnes is found in hair follicles (pilosebaceous glands) especially around the shoulder area, and is more commonly found in men than women.6 P. acnes are small-to-medium Gram-positive rod-shaped bacteria that exhibit facultative anaerobic metabolism.7 8 This organism is primarily known for being involved in the pathogenesis of chronic inflammatory acne and other chronic conditions or infections such as prosthetic shoulder and hip infections, silicone breast prosthetic infections, endocarditis of prosthetic and native aortic valves, corneal infections, postoperative endophthalmitis, focal intracranial infections, cerebrospinal fluid shunt infections and sarcoidosis.8
In orthopaedics, P. acnes has become notorious as an indolent and often difficult to diagnose opportunistic pathogen in spine and shoulder infections. This likely reflects the proximity of these sites to areas where there are relatively high concentrations of pilosebaceous glands. For example, Propionibacterium have become the most common bacteria to be recovered at surgical revision of a failed shoulder arthroplasty.9 P. acnes are a much less common cause of infection in elbow prosthetic arthroplasty, likely reflecting the very low prevalence of this organism in the cutaneous tissues of the elbow.10 Somerson et al10 reviewed 20 studies that reported deep infection rates after total elbow replacement. Of the six studies that reported organisms grown on culture (1667 cases), P. acnes only represented 0.7% of the infected cases (11 of 1667 cases).
Similar to our patient’s case, the onset of infection with P. acnes is usually insidious and of low virulence, and once established it persists due to the tendency of these organisms to form a biofilm.7 For this reason, antibiofilm antibiotics, such as rifampicin (rifampin), are often necessary for successful treatment.7 However, rifampicin-resistant P. acnes have been known to appear as a result of this treatment.11 High dose intravenous penicillin is usually the drug of choice for treating P. acnes infections and rifampin is often used in combination with this antibiotic or others (eg, vancomycin or daptomycin).4 A main reason that we did not use penicillin and rifampin is that during the final phase of our patient’s treatment we were primarily concerned for Gram-positive coverage and a polymicrobial infection. It is for this reason that we used piperacillin/tazobactam and vancomycin.
Improvements in isolating P. acnes can be achieved when employing the advanced methods. For example, in a prospective multicentre study of prosthetic joint infections, Bémer et al12 showed that P. acnes infections were most reliably detected using Schaedler broth (up to 14 days incubation time). ESR and CRP levels are also known to have poor sensitivity for the diagnosis and monitoring of the progress of the treatment for infected shoulder prosthetic arthroplasties.13 This is consistent with the variable ESR and CRP levels in our patient throughout the course of his illness and the failure of these markers to completely normalise by the end of his treatment.
P. acnes can remain viable on inanimate object surfaces for at least 17 days.14 While it might be conceivable that the organism was present on the metal rail at the time the patient struck it with his left elbow, it is more likely that this organism was present on his skin, especially given the presence of S. epidermidis in the same culture. Nevertheless, P. acnes are rarely the cause, or detected as a contaminant, in cases of infected olecranon bursitis. This is supported by our failure to find any reported cases of these associations in our literature searches.
Predisposing factors that increase the risk of acquired septic olecranon bursitis are persistent pressure on the bursa (eg, due to work demands), corticosteroid therapy, rheumatoid arthritis, lupus, gout and other conditions that reduce immunity. As a child our patient had poliomyelitis, which could increase the potential for opportunistic infections due to an ‘immunocompromised cutaneous district’ because the virus has been shown to result in regional impairments in nerve conduction that could lead to decreased peptidergic stimulation of immunocompetent cells.15 Although poliomyelitis primarily affects motor neurons, there is evidence that sensory neurons are also impaired. The novel concept of a selectively diminished cutaneous and subcutaneous inflammatory response due to regional poliomyelitis-related nerve damage is further supported by case reports that detail the sparing of a poliomyelitis affected limb from psoriasis, joint sparing in a patient with unilateral psoriatic arthritis with a history of hemiplegia, and sparing of limbs affected by past infection with poliomyelitis in patients with systemic sclerosis.16 However, although our patient’s poliomyelitis infection did permanently affect the joints of his upper extremities (primarily with mild elbow contractures), there is no clear evidence that his chronologically remote polio infection contributed to his P. acnes olecranon bursitis. A link between his P. acnes olecranon bursitis/osteomyelitis also seems unlikely because he did not have any prior history of atypical or unusual infections.
Patient’s perspective
I am pleased with the final outcome, but in the first 3–4 weeks it was clear that the antibiotics choices were not working. I am grateful to return to swimming and all work-related activities.
Learning points
Propionibacterium acnes and Staphylococcus epidermidis can be rare pathogenic causes of olecranon bursitis and osteomyelitis due to their ubiquitous presence on the skin.
Wound cultures taken in these conditions must be held for adequate time to detect growth of these organisms and guide appropriate treatment decisions.
Penicillin-based antibiotics with a beta-lactamase inhibitor provide coverage for P. acnes and is a viable treatment option for bone and soft tissue infections with this pathogen.
References
Footnotes
Contributors All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole and have given final approval to the version to be published. All the authors were involved in the conception and design of the case report after seeing the patient throughout the course of his care. Each author assisted in the drafting and revision of the article and approved the final version. All authors also agree to be accountable for the article and will ensure that questions regarding the accuracy or integrity of the article are resolved.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.