Article Text

Statistics from Altmetric.com
Description
We report a case of a 4-week-old female neonate who was admitted to the hospital for a anterior right lump of the neck, perceived by his mother the day before. The mother also noticed a preferential tilting of the head towards right. He was an otherwise full-term healthy baby, with a history of instrumented delivery. There was no fever, trauma or respiratory symptoms/signs. Family history was irrelevant. On examination, the neck swelling was a small firm, partially mobile, no warm on touch and apparently painless mass, with approximately 1.5–2 cm soft tissue mass, attached to the right sternocleidomastoid muscle. There was no restriction of neck movements. Ultrasonography (USG) revealed a 13 mm fusiform thickening of the right sternocleidomastoid muscle, with maintained structure of muscle fibres (figures 1 and 2). No cervical lymphadenopathy, signs of infiltration or other anomalies were found (figures 1 and 2). Both clinical and radiological findings favoured the diagnosis of fibromatosis colli. The parents were advised to perform adequate stretching exercises on the neonate, and she was referred to physiotherapy for follow-up. At present, after 4 weeks, the neck swelling showed slight decrease in size with near normal neck movements.
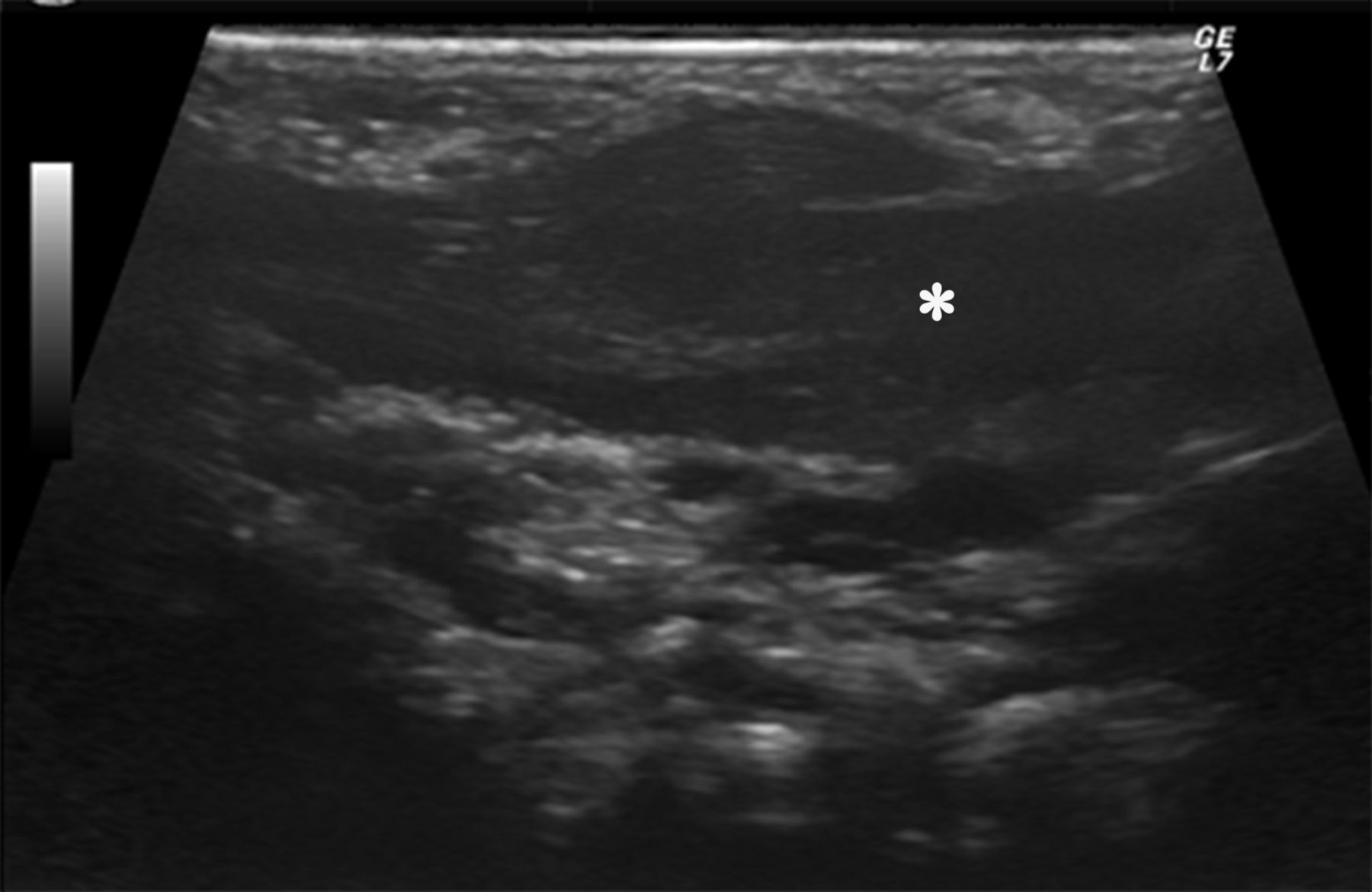
Ultrasound showed a diffusely enlarged right sternocleidomastoid muscle having a fusiform shape in a 4-week-old female neonate (asterisk). These features were consistent with fibromatosis colli.
{kind=link}
{kind=link}
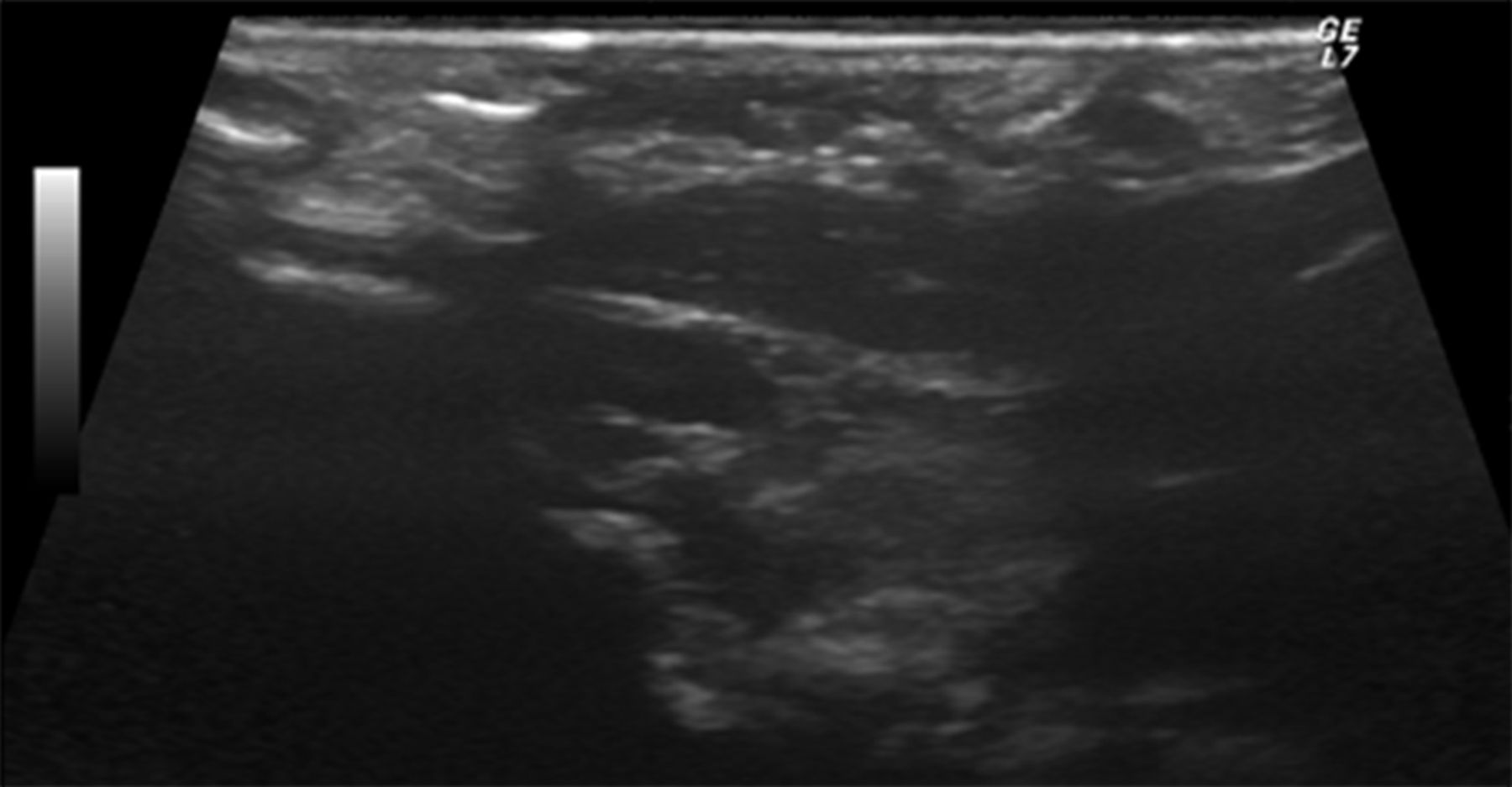
The left sternocleidomastoid muscle appeared normal.
Fibromatosis colli has a prevalence of 0.4%, with male predominance.1 It is a congenital benign fibrous tumour developed from the sternocleidomastoid muscle.1 It manifests clinically by neck swelling and movement restriction (torticollis).2 The exact aetiology is unknown, but it is attributed most of the time to ischaemia of the muscle after difficult or forceps delivery.2
USG is the imaging modality of choice.1 3
The differential diagnosis for a neonate presenting with a neck swelling or mass can be diverse. These may include benign lesions, such as cervical lymphadenopathy and branchial cyst, which have a particular clinical picture and radiological signs, and rhabdomyosarcoma, neuroblastoma and lymphoma, in which, in addition to a neck mass, there can be enlarged cervical lymph nodes, vascular encasement or invasion of surrounding structures.1 3
Treatment is based on physiotherapy and should be begun early to ensure a better outcome.1
Learning points
This case illustrates the essential clinical features of fibromatosis colli, a relatively rare cause of neck mass.
Ultrasonography is the preferred diagnostic tool due to low cost and absence of ionising radiation. It also has a sensitivity of 100%. In the appropriate clinical setting, it is sufficient to establish the diagnosis with a high degree of confidence, avoiding unnecessary investigation procedures which in turn can increase parental anxiety.
Treatment is mainly conservative, consisting in most cases of passive or active physiotherapy, with required surgical intervention in <10% cases.
Footnotes
Contributors JCO: patient’s diagnosis and treatment, discussion of conduct, follow-up of the patient, conception and design, acquisition of data, literature research and conception of the paper and revision of the final version of the article. MSA: patient’s diagnosis and treatment, discussion of conduct, follow-up of the patient, conception and design, acquisition of data, literature research and conception of the paper. FMG: acquisition of data and conception of the paper.
Competing interests None declared.
Patient consent Guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.