Article Text

Statistics from Altmetric.com
Description
An 88-year-old bedbound woman from a nursing home with a background of dementia was transferred by ambulance to accident and emergency with abdominal distension, pain and a decreasing level of consciousness. On examination the patient was feverish, hypotensive and tachycardic, consistent with sepsis. The abdomen was distended, with tenderness and guarding at the paraumbilical area. Digital rectal examination showed faecal loading. She was resuscitated with intravenous fluids, and blood results showed a raised lactate (4.1 mmol/L), acute kidney injury and raised inflammatory markers (white cell count 9.1×109/L and C reactive protein 410 mg/L). A chest X-ray did not demonstrate any free air under the diaphragm, and abdominal X-ray showed a large air shadow in the centre of the abdomen (figure 1).

Plain abdominal X-ray showing a large central air pocket.
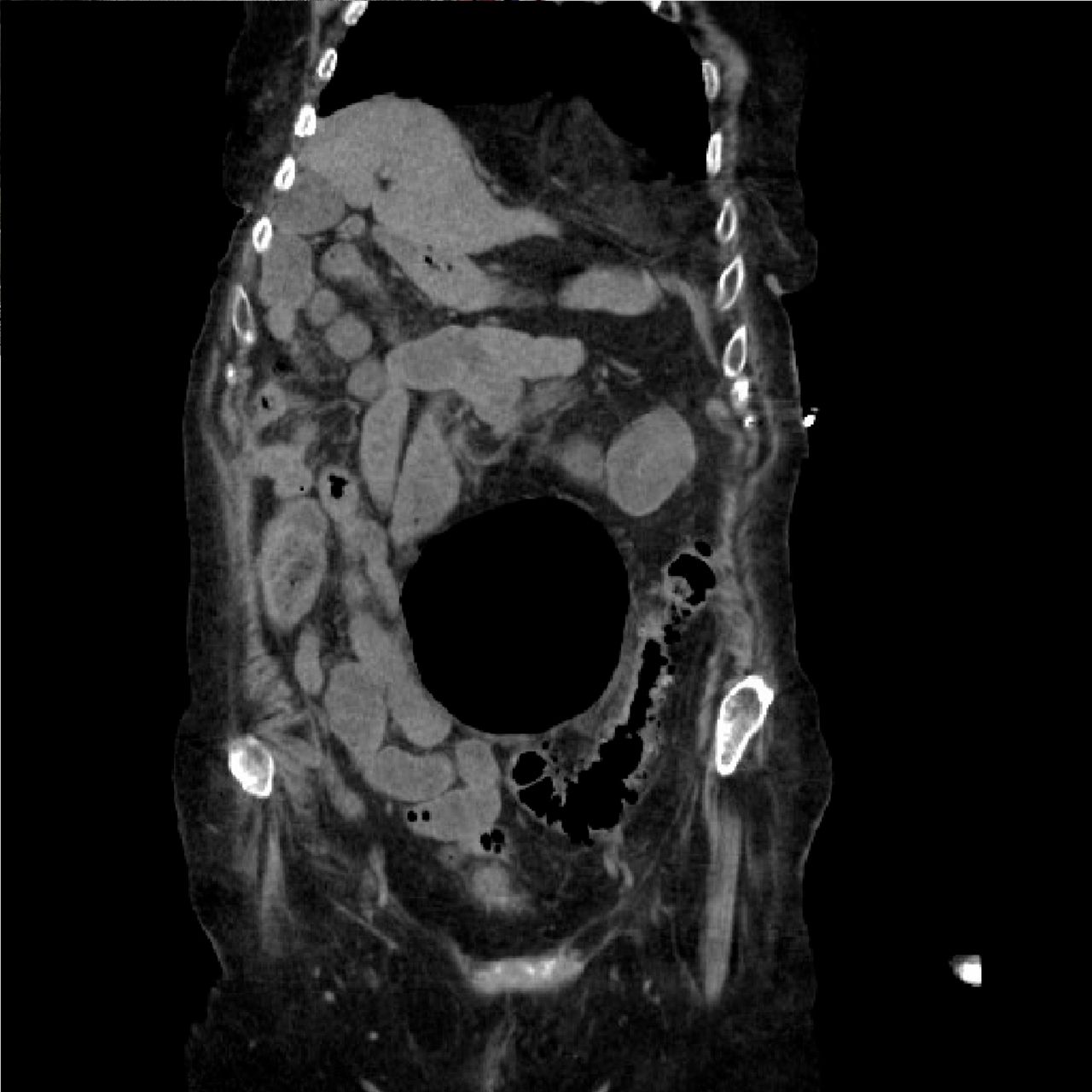
The working diagnosis was a localised perforation, and therefore a CT scan of the abdomen and pelvis was urgently arranged. The CT demonstrated one large air-filled outpouching (11×6 cm) anterior to the sigmoid colon (figure 2), which was initially (prior to a formal radiology report) thought to be a contained bowel perforation, although there was no evidence of any other pockets of free air in the abdominal cavity. After review of the images by a consultant radiologist, the CT was reported as a giant sigmoid diverticulum (figures 3 and 4) originating from the sigmoid colon, with inflammatory changes suggestive of acute diverticulitis. The patient was managed conservatively with intravenous fluids and antibiotics.

Axial CT image showing a 11×6 cm giant diverticulum.

Sagittal CT image showing the giant diverticulum anterior to the sigmoid colon.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coronal CT image showing the giant diverticulum.
Learning points
Giant colonic diverticulum (GCD) is rare, with less than 200 cases reported in the literature.1
The CT findings of large diverticulum can be mistaken for a contained bowel perforation, and it is important to differentiate between the two pathologies as their managements can be different.
GCD can be complicated by volvulus, bowel obstruction, perforation, abscess formation, sepsis and rectal bleeding.2 3
Two per cent of giant diverticulum is associated with malignancy, either within it or distal to it, so it is important to arrange flexible sigmoidoscopy before elective bowel resection.2 However, a clear causal association between giant diverticulum and malignant transformation has yet to be established.
Although conservative management is possible for high-risk surgical patients (as in this case), surgical resection of the diverticulum is the mainstay of treatment for GCD.3 A review of 16 cases of GCD treated with sigmoidectomy and en bloc resection of the diverticulum reported no postoperative deaths and a morbidity rate of 6%.1
Due to the risk of complications from GCD and the low reported morbidity and mortality from their surgical resection, elective surgery could be considered as a management option for uncomplicated GCD.
Footnotes
Contributors Initial idea by AM. AM and SL contributed to the first draft and acquisition of data. Consent was obtained by SL. AM and SL wrote and agreed on the final draft.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.