Article Text

Statistics from Altmetric.com
Description
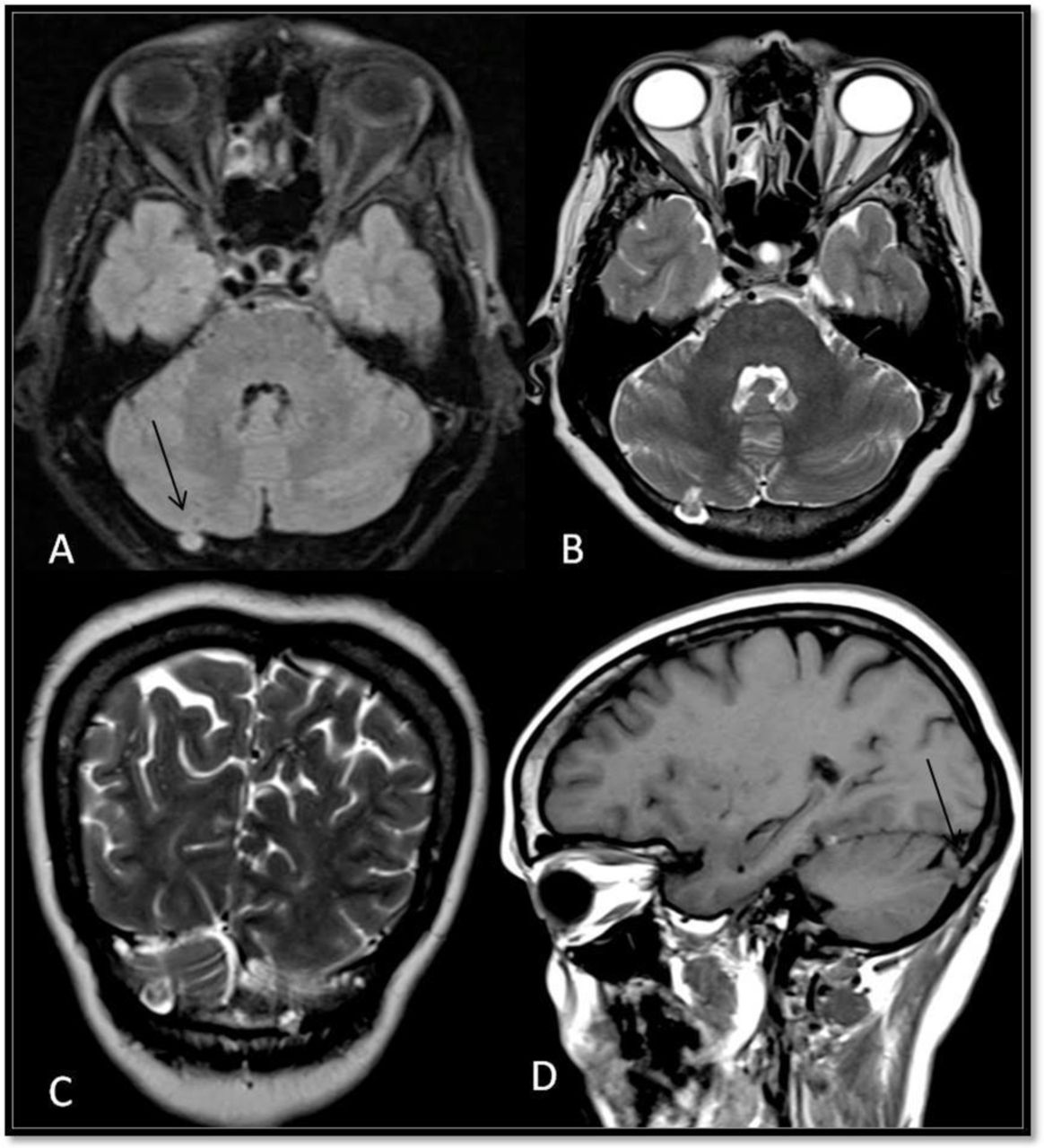
A 52-year-old woman presented with complaints of non-specific headache. The patient had a history of head injury 1 year ago. Clinical neurological examination was nil significant. The skin over the occipital region is normal. No prior investigations were done immediately after the injury. MRI of the brain at present showed small intradiploic cerebrospinal fluid (CSF)-filled defect with herniation of foliae of the right cerebellar hemisphere (figure 1). The rest of the brain parenchyma revealed no abnormality and no skull fracture was seen. Features were suggestive of intradiploic cephalocele involving cerebellar foliae.

{kind=link}
Axial Fluid attenuated inversion recovery (A), T2 (B), coronal T2 (C) and sagittal T1 (D) images at the level of the cerebellum showing small calvarial defect in the occipital bone on the right side with intradiploic herniation of the right cerebellar foliae (black arrows).
A cephalocele is defined as protrusion of intracranial content through a defect in the skull. The herniating tissue may be meninges, brain, CSF and vascular structures. Various causes that lead to cephalocele include infection, trauma, surgery and tumours, and can be congenital.1 Cephaloceles of the cranial vault are a rare complication of skull fractures. The patient may present with painless/painful subcutaneous swelling. Parietal location is the most common site for congenital cephaloceles.2 Intradiploic cephaloceles can be congenital or acquired. Our case demonstrates a rare location of intradiploic cephalocele presenting with non-specific symptoms, which may not be related to trauma as there were no fracture and structural lesion. Majority of cephaloceles with large calvarial defect require dural repair.
Learning points
Cephaloceles are classified by Shi et al,3 based on location as basal, sincipital, convexity and atretic types.
Intradiploic cephalocele can simulate as a lytic lesion, which can resemble eosinophilic granuloma, metastases, dermoid cyst and haemangioma.
Cerebrospinal fluid within the lesion, disruption of the inner table, integrity of the outer table and demonstration of the presence of herniated brain parenchyma are characteristic findings of intradiploic cephalocele.
Footnotes
Contributors MV: conception and design, acquisition of data, or analysis and interpretation of data. SVC: drafting the article or revising it critically for important intellectual content. UBS: agreement to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved. PPN: final approval of the version published.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.