Article Text

Summary
A 43-year-old woman with a history of recently diagnosed metastatic melanoma was commenced on systemic therapy with nivolumab, an anti-programmed cell death-1 monoclonal antibody and one of an increasing group of the so-called ‘immune checkpoint inhibitors’. She experienced a dramatic complete response within 6 months of initiation. However, in addition to developing incident autoimmune hypothyroidism, she also developed progressive fatigue, proximal weakness, myalgia and dysphagia. Initial investigations with blood tests, electrophysiology and a muscle biopsy were non-specific or normal. Subsequent examination revealed ‘woody’ thickening of the subcutaneous tissues of the forearms, thighs and calves consistent with fasciitis. MRI and a full-thickness skin–muscle biopsy were ultimately diagnostic of a likely iatrogenic autoimmune myofasciitis. The clinical manifestations only responded partly to prednisolone 30 mg orally and treatment was escalated to include intravenous immunoglobulin. At 3 months, this has only resulted in a modest incremental improvement.
- musculoskeletal and joint disorders
- muscle disease
- oncology
- unwanted effects / adverse reactions
- musculoskeletal syndromes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- musculoskeletal and joint disorders
- muscle disease
- oncology
- unwanted effects / adverse reactions
- musculoskeletal syndromes
Background
The use of immune checkpoint inhibitors represents a paradigm shift in the treatment and prognosis of an increasing range of malignancies and is providing insights into the shifting horizon between malignancy and autoimmunity. By unleashing naturally occurring antitumour responses via blocking T-cell negative costimulation, targeting anti-programmed cell death-1 (PD-1) and its ligand (PD-L1) has revolutionised outcomes in an increasing range of malignancies. Monotherapy response rates in metastatic melanoma are around 40% and they can be durable, lasting long after therapy has ceased.1 However, intuitively when considering their mechanism of action, immune-related adverse events (irAEs) are common and have been described to affect almost every organ system.2 Of particular relevance to this case, irAEs with rheumatic or musculoskeletal disease phenotypes are becoming increasingly recognised and are likely to grow in incidence as indications broaden and combination regimens become more commonplace.3 Awareness of the potential of these novel therapies to cause such varied presentations should continue to be disseminated among the wider medical community.
Case presentation
We describe a 43-year-old female patient with metastatic melanoma who had a primary melanoma excised from the anterior neck at the age of 18. She had no other prior illness and no family or social history directly relevant to her recent symptoms. Sixteen years later, in December 2011, she was diagnosed with a BRAF-V600E-mutation-positive melanoma in the right inferior rectus muscle without evidence of other distant metastases. Neoadjuvant vemurafenib (a BRAF inhibitor), subsequent combined transorbital and transcranial exenteration of the right eye socket, followed by local radiotherapy was instigated. In May 2013, she presented with a painless firm swelling in her right thigh that was found to represent a further temporally isolated metastatic deposit and was resected. In June 2015, she presented with proximal small bowel obstruction. During surgery, a metastasis was identified as the cause of the obstruction and, additionally, a number of abnormalities were noted to be suspicious for mesenteric tumour deposits. Subsequent restaging showed widespread pulmonary and mesenteric metastases. Her serum lactate dehydrogenase level was normal.
After consideration of her options for systemic treatment, she commenced nivolumab, an anti-PD1-antibody, 3 mg/kg intravenously fortnightly in July 2015. There was a dramatic reaction with a complete response, the absence of any detectible metastatic disease, documented in January 2016. Around this time, she developed autoimmune thyroiditis, subsequently managed with thyroxine replacement.
In September 2016, she developed progressive fatigue and a widespread myalgia affecting both upper and both lower limbs. This was associated with progressive proximal weakness that increasingly interfered with her mobility and with activities of daily living. Additionally, she developed a progressive dysphagia, predominantly affecting solid foodstuffs, and unintentional weight loss. There was no evidence of disease progression, occult infection, cardiac failure or new endocrinopathy to account for these new symptoms. At this stage, her creatine kinase (CK) was normal (75 U/L; <295). An irAE was suspected and oral prednisolone 30 mg daily commenced while awaiting further investigation results.
Investigations
An electromyogram showed only borderline myopathic features in the proximal muscle groups without evidence of a peripheral neuropathy or neuromuscular junction disorder. A percutaneous tibialis anterior muscle biopsy showed no significant abnormality. Her symptoms improved on prednisolone to the point where she could mobilise but continued to struggle rising from a seated position and with eating.
She was referred to neurology and rheumatology services who sought to further characterise the likely irAE. She did not complain of fevers, rash or relevant other associated connective tissue disease symptoms. On examination, the skin over her forearms, calves and chest had a ‘woody’ feel without tendon crepitus but with contracture affecting the left forearm flexor compartment. There was no distal skin thickening, no telangiectasia or other systemic sclerosis stigmata and no macroscopic nailfold capillary abnormality. Proximal power was reduced bilaterally (Medical Research Council (MRC) grade 4/5 power). Further investigations were organised.
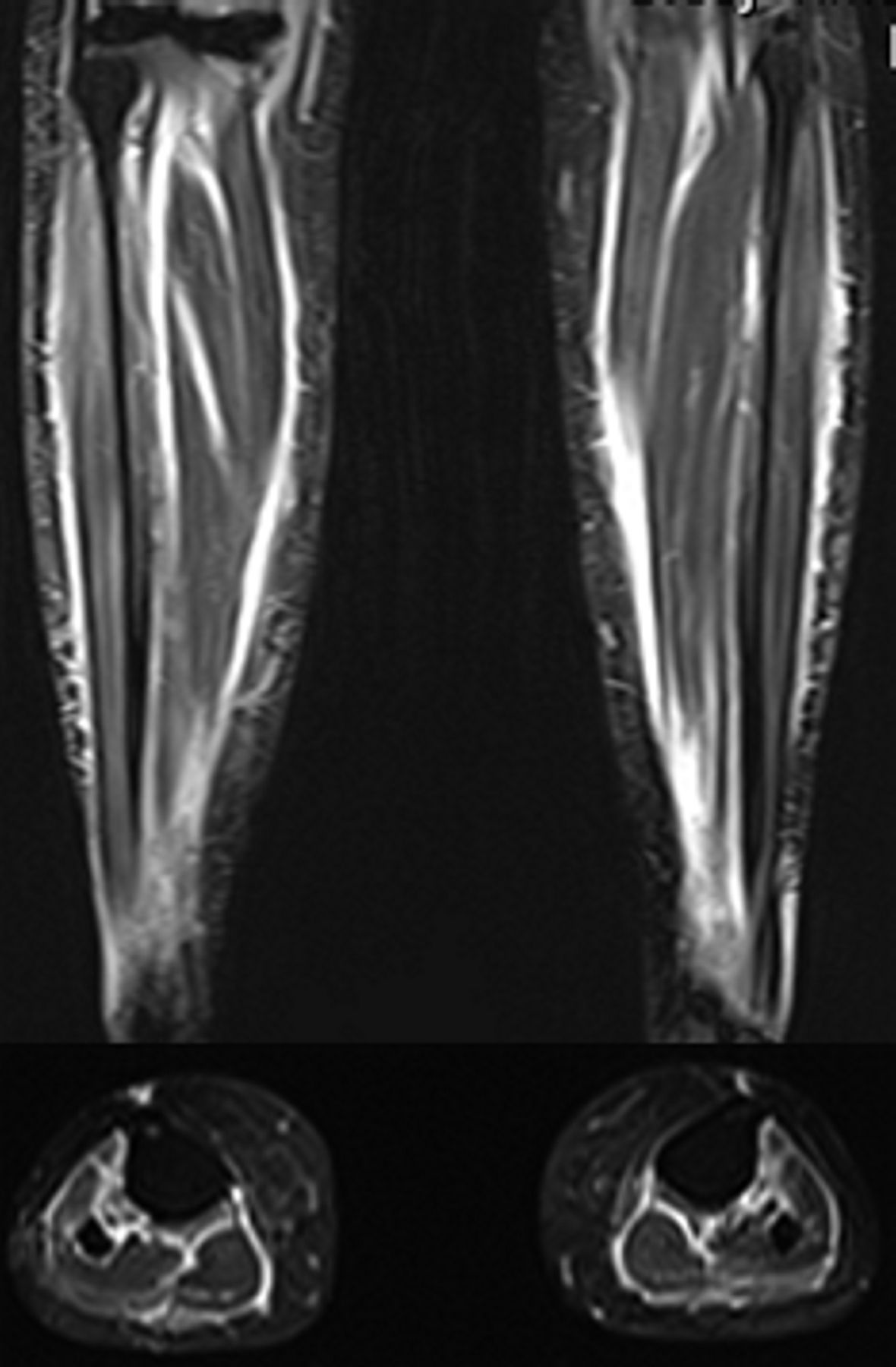
Blood tests revealed a persistently normal full blood count, including a normal eosinophil count, and CK. An extended immunological screen for overlap connective tissue disease and myositis-specific and associated antibodies was negative. MRI studies showed striking abnormalities; however, with symmetric fascial thickening and intense short-tau inversion recovery, signal centred around the muscle fascia of all thigh and calf muscle groups (figures 1 and 2). A subsequent full-thickness skin–muscle biopsy demonstrated a focused fascial and perifascicular inflammatory infiltrate (figure 3). A majority of myofibres showed Human Leukocyte Antigen (HLA) Class-I immunolabelling, again with perifascicular accentuation. These histological features helped to confirm the working diagnosis of myofasciitis.
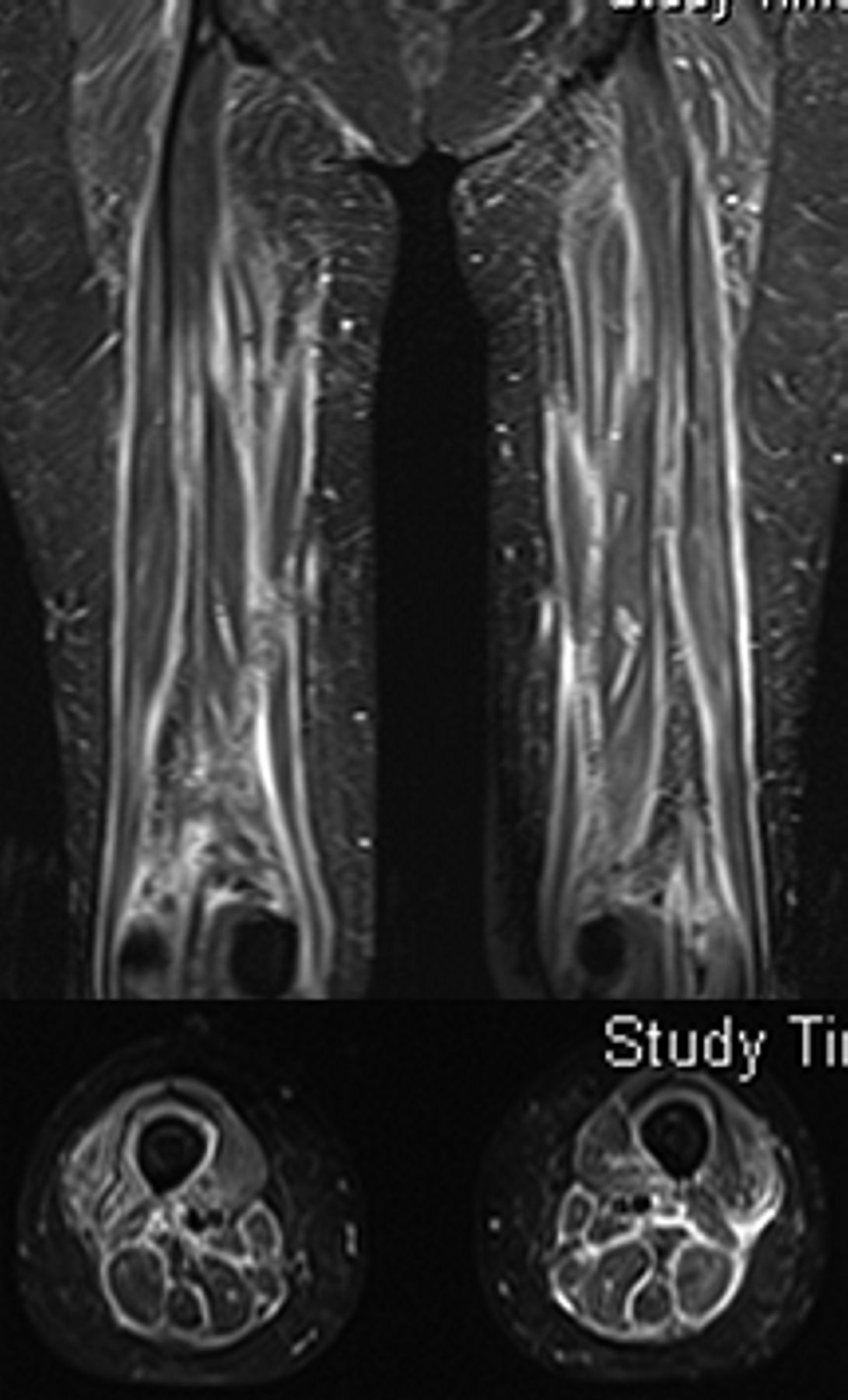
Coronal and representative axial T2 short-tau inversion recovery sequence MRI images of both thighs demonstrating marked signal hyperintensity in a perimysial and perifascicular distribution, consistent with fasciitis.
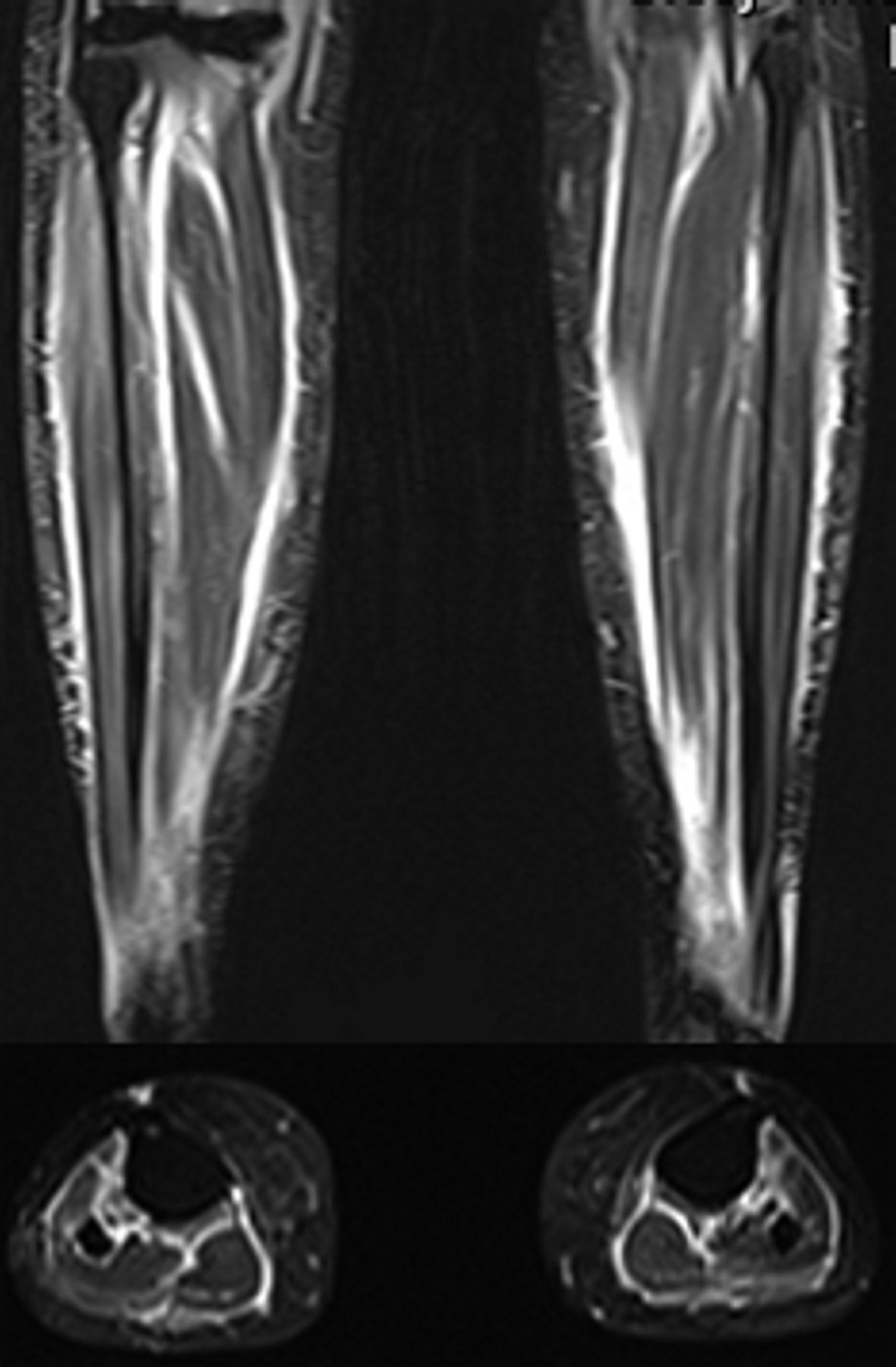
Coronal and representative axial short-tau inversion recovery sequence MRI images of both calves again demonstrating marked signal intensity in a perimysial and perifascicular distribution consistent with fasciitis.

{kind=link}
{kind=link}
{kind=link}
CD3 immunostaining (original magnification ×100) of right thigh full-thickness biopsy demonstrating T-lymphocyte-mediated inflammation preferentially affecting fascia (above right) with minimal endomysial activity present in perifasicular muscle (below left).
Differential diagnosis
Although the suspicion from the outset of her presentation in September 2016 was that an irAE triggered by the nivolumab was the cause of her symptoms, it took an extended work-up to fully characterise the clinical phenotype. Initially, given the presentation with weakness and myalgia, investigations were targeted towards investigating possible inflammatory myopathy, neuropathy or a neuromuscular junction disorder. However, the normal CK, the non-specific electrophysiology and normal muscle biopsy suggested against these diagnoses. As her symptoms evolved, the characteristic woody thickening of the subcutaneous tissues became evident and prompted the ultimately diagnostic investigations.
Treatment
Given the partially glucocorticoid refractory nature of her symptoms, an escalation in treatment was required. However, there is no guidance or existing literature on the treatment of an autoimmune myofasciitis and, consequently, the treatment options considered were extrapolated from experience with other causes of fasciitis, systemic autoimmune disease and experience with irAEs more generally. The options to combine with the glucocorticoid considered included oral immunosuppression with agents such as methotrexate and mycophenolate, more potent immunosuppression with intravenous cyclophosphamide or immunomodulation with intravenous immunoglobulin (Ig). Intravenous Ig, administered as 2 g/kg monthly, was chosen given its typically rapid onset of efficacy and given the context of active malignancy.
Outcome and follow-up
After three treatment cycles, she has noticed a modest improvement symptomatically in her skin ‘stiffness’ but unfortunately, apart from in grip strength, we have not been able to demonstrate an objective improvement in her other manifestations. Her symptoms have not worsened, however, and she remains in complete response with regards to her malignant melanoma.
Discussion
There are increasing reports covering a spectrum of inflammatory myopathies related to checkpoint inhibitors. However, attributing a causal relationship from these medications is partly hampered by the concomitant association between malignancy and certain myositis subtypes such as dermatomyositis.4 Nonetheless, in this case, the CK remained normal and the initial biopsy did not show evidence to support a myositis. Instead, the symptoms of prominent myalgia, unusual for an isolated myositis,5 along with the subsequent clinical findings of woody subcutaneous tissues, the MRI findings and the full-thickness biopsy ultimately helped confirm the clinical suspicion of myofasciitis. Of additional relevance to the differential diagnosis is a case series of two patients diagnosed with systemic sclerosis attributed to pembrolizumab therapy (another PD-1 inhibitor).6 These cases shared some clinical features such as skin thickening, although this did involve the extremities in contrast to our case, and were both seronegative for autoantibodies, as in our case.
There has been one case of eosinophilic fasciitis described associated with pembrolizumab (another PD-1 inhibitor) in a 51-year-old woman after 18 months of treatment.7 As in this case, the CK was not significantly elevated but, in contrast, the patient had a marked peripheral eosinophilia (5.24×109/L; 0.04–0.4) and biopsy findings were of a predominantly eosinophilic infiltrate. A clinical vignette has been very recently published of a 64-year-old man receiving nivolumab for renal cell carcinoma who developed a myofasciitis. He experienced extensive tendon crepitus and his symptoms quickly resolved with a short course of methylprednisolone in contrast to the experience of our described patient.8
Fasciitis itself has a range of causes with infection (often termed ‘necrotising fasciitis’ in the literature), regional syndromes (such as plantar fasciitis or nodular fasciitis) and eosinophilic fasciitis the most common. Other reported associations include malignancy, granulomatous conditions and autoinflammatory syndromes.9 The cause of myofasciitis in this case is not clear, but its temporal link to checkpoint inhibition while the tumour burden was in clear regression led us to the conclusion that it was likely iatrogenic.
Our patient with autoimmune myofasciitis adds to the spectrum of autoimmune rheumatic diseases triggered by checkpoint inhibition and should alert the reader to development of such symptoms in similarly treated patients.
Learning points
Programmed cell death-1 is a T-cell negative costimulatory molecule, blocking its actions with an expanding class of medications known as immune checkpoint inhibitors promotes certain naturally occurring anticancer effects.
The applications for immune checkpoint inhibitors are rapidly broadening in parallel with an increasing incidence and spectrum of autoimmune-like immune-related adverse events (irAEs).
Prominent myalgia is unusual for an isolated inflammatory myositis and implies involvement of the fascia in addition, or as in this case exclusive, to the myofibres.
Careful reporting and dissemination of irAEs will help to inform judgement of risk and benefit decisions in patients with certain malignancies and encourage early recognition and intervention.
Footnotes
Contributors MJSP was involved in the conception and design, acquisition of data, drafting the article and final approval of the version published. MER, PCL, DGdP and HC were involved in the conception and design, revising the manuscript critically and in the final approval of the version published.
Funding PCL received research funding from Bristol-Myers Squibb
Competing interests PCL has acted as a paid consultant and has received support for travel from Bristol-Myers Squibb.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.