Article Text

Summary
A 32-year-old man born with double inlet left ventricle (DILV) and other significant cardiac abnormalities underwent surgical palliation at 1 day, 2 years and 20 years, before receiving a donor heart at 29 years. To our knowledge, there are no case reports or cohort studies of the effect of exercise training on exercise capacity and peak oxygen uptake (VO2peak) following heart transplantation (HTx) for individuals born with DILV. The patient accessed our clinical exercise physiology service for assessment, advice and support for exercise training over a 7-year period spanning pre-HTx and post-HTx. An individualised exercise plan, together with careful assessment and monitoring, and the patient’s own motivation have contributed to him achieving an outstanding post-HTx doubling of VO2peak and exercise capacity.
- heart failure
- congenital disorders
- rehabilitation medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Patients with congenital heart disease (CHD) comprise approximately 2% of all heart transplantation (HTx) recipients and 11% of HTx recipients aged 18–39 years, the age group of the case reported here.1 Double inlet left ventricle (DILV) describes a congenital syndrome of severe complex heart malformations that carries a high risk of mortality and often requires surgical palliation for symptomatic relief and survival.2 Patients with DILV with significant haemodynamic compromise often progress to HTx.3 4 Peak oxygen uptake (VO2peak) and exercise capacity are strong predictors of survival in HTx recipients in general5 6 and provide a rationale for encouraging exercise training.7–9 Kaplan-Meier survival curves illustrate lower mortality outcomes for paediatric HTx recipients, compared with patients who receive their hearts as adults,1 but there has been a recent narrowing of this difference.1 Patients with CHD who undergo HTx have some of the best survival rates of all HTx patients.1
To our knowledge, there are no published data on the effects of exercise training on VO2peak and exercise capacity for patients with DILV before and after HTx. HTx in the absence of exercise rehabilitation only partially restores VO2peak, physical function and quality of life in patients with severe acquired adult heart failure.10 11 Although some improvement in VO2peak soon after HTx has been widely reported, VO2peak is typically lower in post-HTx patients who do not exercise, compared with those who do.12 13 Studies in paediatric14 and adult HTx15 16 cohorts have reported post-HTx gains in VO2peak to be modest in the absence of exercise, and appear to reverse somewhat in long-term follow-up. For these reasons, long-term exercise participation should be part of routine post-HTx management to try to improve and then preserve VO2peak.5 12 There are some data showing that younger HTx recipients achieve greater improvements in VO2peak with exercise training, compared with older recipients.17
Possible mechanisms limiting full restoration of physical function following HTx comprise central factors including chronotropic incompetence,9 diastolic dysfunction9 18 and coronary artery vasculopathies9 19 and peripheral factors including heart failure-related myopathies,18 microvasculature deficits9 18 and metabolic impairments that mimic the effects of severe detraining.18 Immunosuppressive drugs are also significant co-contributors to exercise limitations after HTx.9 18 There is evidence that endurance and resistance training programmes may reverse at least some of these deficits and should be part of overall management.7 12 15 16 20
The case described here is of an individual born with DILV and other cardiac abnormalities where a major focus was on trying to improve and then sustain exercise capacity following HTx. Prior to HTx, the patient had never been able to engage in sufficient health-promoting exercise. His exercise capacity was measured at regular intervals for several years both before and after HTx, with a total follow-up period of 7 years.
Case presentation
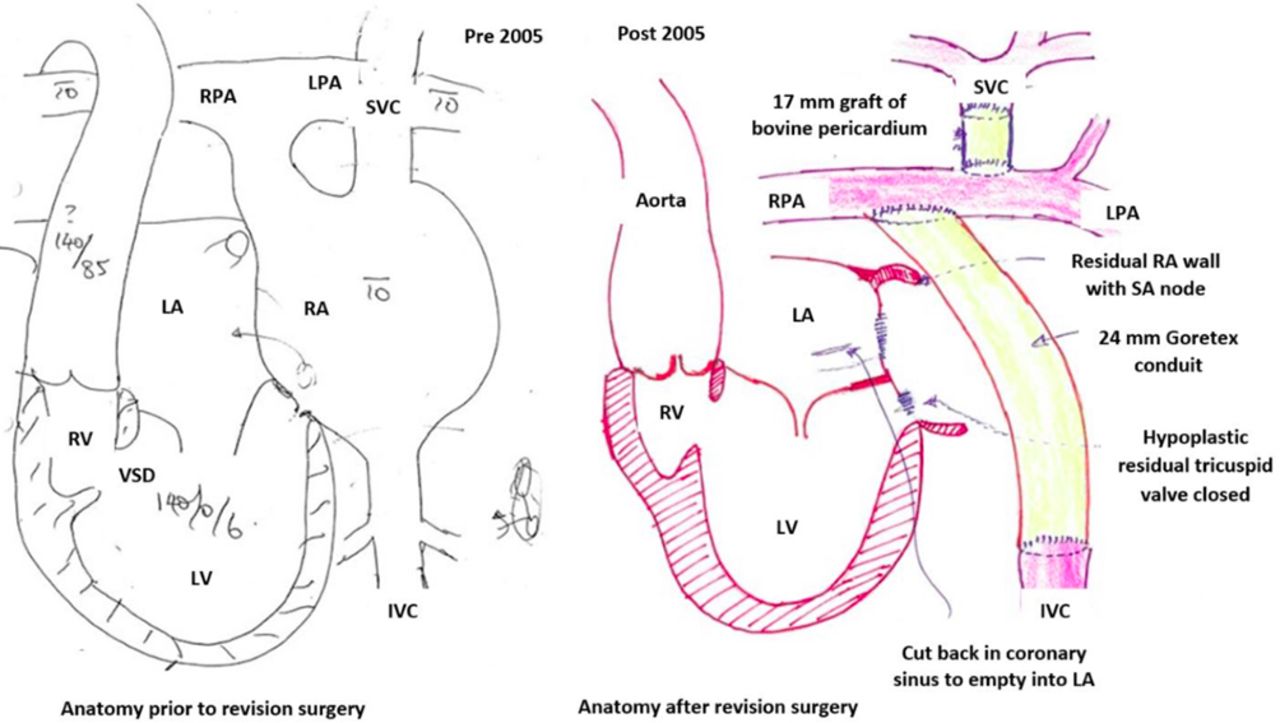
We present a case of a 32-year-old man born with DILV, ventricular septal defect connecting LV to a rudimentary right ventricle, pulmonary atresia, global systolic dysfunction, aortic regurgitation, dextrocardia and situs inversus. At 1 day, he underwent a Blalock-Taussig shunt for cyanotic relief. At 2 years, he underwent an atriopulmonary Fontan procedure where blood flow from his bulbous left-sided right atrium (RA) was shunted to the right pulmonary artery (PA) to improve pulmonary circulation (figure 1A). At 20 years, he underwent a Fontan revision which comprised a 24 mm Goretex conduit connecting inferior vena cava to the right PA, a 17 mm bovine pericardium conduit from superior vena cava to the left PA and excision of most of RA except for the remnants of sinoatrial node (SAN) (figure 1B). The hypoplastic tricuspid valve was closed which completed a series connection of pulmonary and systemic circulations. Excision of RA required the coronary sinus to drain into left atrium (LA). A dual chamber pacemaker was fitted.

(A) Surgeon’s sketch and notes of the heart and great vessels prior to the Fontan revision surgery in 2005 when the patient was 20 years. The conduit between the right atrium (RA) and right pulmonary artery (RPA) was created during the atriopulmonary Fontan procedure at 2 years in 1987. Numbers represent systolic/diastolic pressures (mm Hg). Numbers with bars represent mean pressures (mm Hg). (B) Surgeon’s sketch and notes of the heart and great vessels following the Fontan revision surgery at 20 years in 2005, consisting of a 24 mm Goretex conduit connecting inferior vena cava (IVC) to RA, a 17 mm bovine pericardium conduit from superior vena cava (SVC) to left pulmonary artery (LPA) and excision of most of RA except for the remnants of sinoatrial node. The hypoplastic tricuspid valve was closed which completed a series connection of pulmonary and systemic circulations. Excision of RA required the coronary sinus to drain into left atrium (LA). LV, left ventricle; RV, right ventricle; VSD, ventricular septal defect.
The patient first accessed our exercise physiology service in 2009 (24 years) and presented with symptoms of exercise intolerance and severe shortness of breath on exertion (New York Heart Association class III; LV ejection fraction at this time was 15%) and occasional exercise-related presyncope. An incremental cycle ergometer test was performed and his peak power output and directly measured VO2peak were 100 watts (W) and 16.9 mL/kg/min, respectively. We also estimated his VO2peak to be 15.6 mL/kg/min using a validated predictive algorithm.21 His resting O2 saturation was slightly low at 93% due to coronary sinus insertion in the LA. He desaturated a little further to 89% at peak exercise. There was no clinical evidence of impaired pulmonary diffusing capacity, nor evidence of ventilatory limitations based on spirometry at rest and during exercise. His pre-exercise, exercise and recovery blood pressures were moderately low, for which he was prescribed an inotrope, while his pacemaker did not respond to exercise, with heart rate (HR) fixed at 80 beats per minute throughout pre-exercise, exercise and recovery (figure 2). This, together with severe heart failure, indicates that he relied primarily on peripheral ‘non-cardiac’ factors (oxygen extraction), rather than inotropic and chronotropic activity as the main contributors to VO2peak, consistent with a recent review on mechanisms of impaired pulmonary VO2 in patients with heart failure and reduced ejection fraction.22

{kind=link}
{kind=link}
Heart rates (HRs) at rest and during incremental cycle ergometer protocols for 2009 and 2010 (pre-transplant) and 2015 and 2016 (post-transplant). His heart was paced a constant 80 beats per minute throughout 2009 and 2010 and did not respond to exercise. The HR data at rest and peak exercise were collected for the 2011 test (see table 1), but the incremental HRs were not archived.
Outcome and follow-up
The main outcome measures for the series of exercise assessments before and after HTx (2009–2016) are summarised in table 1 and figure 2. At first, we recommended swimming (horizontal, weightless exercise) to promote venous return and pulmonary circulation, but he did not enjoy swimming due to very rapid fatigue. He preferred dancing and this was his main active recreational pursuit, but he fatigued rapidly and needed to rest for long periods between short bursts of dancing.
Main outcome measures for a series of exercise assessments for several years before and again after HTx
The cycle ergometer assessment was repeated in 2010 and 2011 (table 1) before he deteriorated to the extent of not being able to attend the exercise physiology service (2012–2014). He underwent HTx at the age of 29 years in 2014. HTx is relatively common in DILV patients with poor haemodynamics.3 Following HTx and several months of cardiac rehabilitation, we designed a multimodal exercise plan of aerobic exercise on most days of the week (mainly cycling on both a cycle ergometer and a road bike) and 2–3 sessions per week of resistance exercise training using large muscle groups and increasingly complex movement patterns.
Since transplant, he has made remarkable progress with VO2peak estimated21 to be 23.4 mL/kg/min (150 W peak power) in 2015 and 29.7 mL/kg/min (190 W) in 2016 (table 1). Notably, his improvement in VO2peak (15.6 mL/kg/min representing 97% improvement) is much higher in both actual and percentage terms than some exercise intervention cohort data following HTx,6 13 17 although one factor contributing to this could be his relative youthful age.17 On the other hand, his VO2peak 2 years after HTX reached only about 69% of age-related American College of Sports Medicine (ACSM) norms,23 and this is similar to HTx populations in general. It is possible that his very low VO2peak before HTx and inability to exercise sufficiently for the first 30 years of his life contributed to him not being able to fully restore his VO2peak after HTX to match his age peers. Since HTx, he has gained 4 kg in body mass and he reports significant muscle development especially in the lower limbs. He no longer desaturates and is experiencing a gradual improvement in chronotropic competence,18 24 as evident by lower resting HRs, and lower HRs at the same submaximal work rates in 2016 compared with 2015, while peak HR was higher (figure 2). This is consistent with criteria for functional reinnervation defined by significant increases in HR during exercise of at least 36 beats per minute and rapid falls in HR during recovery.25 The mechanisms for the improvement in chronotropic competence may be associated with partial, progressive cardiac allograft sympathetic reinnervation18 26 27 and he is now unrestricted in exercise participation.
Discussion
To our knowledge, this is the first case report documenting the effects of exercise training on exercise capacity before and after HTx in a patient with DILV. Peak oxygen uptake (VO2peak) and exercise capacity are strong predictors of survival in HTx recipients in general5 6 and this patient was able to double both his peak exercise power and VO2peak at 2 years post-HTx. The improvement in VO2peak is 26% higher than the average improvement reported for 1700 adult heart transplant recipients9 leading to a recommendation that exercise should be part of routine management post-HTX in DILV patients.
Patient’s perspective
From a young age I’d always known that there was something different about me. While I was relatively well when I was young and was able to keep up with the other kids, having to regularly visit doctors and have warfarin blood tests every other week meant I was well aware I was different. However, the seriousness of what was wrong didn’t’ really set in until I was much older.
It wasn’t until I was about 12 years that I had my first serious arrhythmia episode that required cardioversion. Through my teenage years it became much more apparent that there was a difference between myself and my peers. I regularly sat out of physical education classes and just tried to ‘be there’ whenever friends went out or went away. While perhaps not joining in on activities, I’d at least be with my friends.
At the end of my high school years was where my heart finally started to have serious issues with arrhythmias. At the end of my final 2 years of school, I had admissions requiring cardioversion. After the first one, I was told that I would require some sort of interventional surgery, however my cardiologist wanted to wait until I finished my final year of high school. That plan almost worked; however, I ended up having an episode before my final exams which turned into a long-lasting issue of constant arrhythmias and required some stronger medication. Soon after, they determined that I needed major surgery and would need a Fontan revision; however at that time, this surgery had never been done in Australia before, and there was no team available to do such surgery.
I was left for some 18 months in a state of uncertainty as to what was needed. Finally, a team was assembled and I had Australia’s first Fontan revision. In retrospect, the reality is that this surgery didn’t really do much for me. Although it stopped my arrhythmias, it also destroyed my sinoatrial node, and I remained in heart failure with my heart continuing to deteriorate. It wasn’t too long after my Fontan revision surgery that my paediatric cardiologist said to me that he believed that he had done all that he could do for me and referred me to the Heart Failure clinic at the Alfred hospital, for which I would eventually be listed for transplant. I went into a period of a long slow decline which would eventually require a heart transplant. Unfortunately, my heart failure also led to severe kidney dysfunction and liver cirrhosis.
Through the period from the Fontan revision surgery to my transplant listing, I was in a health purgatory, where I was in heart failure and my health was slowly declining over the period of many years. This was in my early 20s, years that were ‘supposed to be’ my best years; however, I became so ill that eventually I got to a point where I had to buy an electric toothbrush because I became too breathless to even brush my teeth.
During the pretransplantation years (2009–2013), I consulted with exercise physiologists who supported me by measuring my fitness and advising me on exercise, although towards the end, it became increasingly difficult to engage in any discretionary exercise.
While I did continue to go out with friends and remain social, this was more about doing it for my own sanity. I developed a coping mechanism where I would choose how and where to expend my energy for the day; for instance, if I planned to go out in the evening, I would rest all day and ‘save’ my energy for that. This was the only way that I could manage to go out for social events. After going out socially at night, it would take at least a day or two to recover.
Once listed for HTx, the wait began. Waiting for a transplant is a very stressful time period. I would visit my doctors every 3–6 weeks depending on how well I was at the time. At every appointment, I would describe how I had been for the last few weeks and then they would nod and say ‘yes well you need a transplant, and that should resolve many of these issues’. But the waiting never seemed to end. Imagine being told to expect the most important phone call of your life, at any time of day but they would not give you any indication of how long it would be until you were called. It could be tomorrow, it could be right this second, it could be in 2 years time. I ended up having serious anxiety on a few occasions when I lost mobile phone reception. Eventually, 865 days passed and I received ‘the call’ at 12:30am on a Friday night. It was both exciting and terrifying.
Recovering from the transplant was a massive challenge. While it is mandated that I participate in a 3-month rehabilitation programme, the first week after the surgery was spent in ICU and I lost around 10 kg of body weight. When I was well enough to start the rehabilitation, I could almost fit one hand around my thigh.
During my first rehab session (which was agony), I saw a young girl running on the treadmill. I was told that she was 8 weeks post double lung transplant, and it was expected that in a similar time frame, I would be running, too. I did not believe the physiotherapists who told me that, but sure enough, I was able to run at about 10 weeks. My rehabilitation was slightly interrupted due to an episode of rejection that needed treatment.
From the end of my formal rehabilitation programme, I continued informal rehabilitation with an exercise physiologist friend, as well as annual exercise tests on a cycle ergometer in order to chart any progress that I was making post-HTx. The exercise physiologist also helped me by prescribing a range of exercise intensities that I could do now, and progressions as I got fitter. The exercise plan consisted of both aerobic exercise (mainly cycling including road cycling) and a progressive strength training plan. At about the 8-month mark, I started on a 5 km running programme. On my 1-year transplant anniversary, I celebrated by running 5 km for the first time in my life with some friends. Running and later riding were things that I never thought or believed that I would be able to do.
Learning points
The patient was born with disabling congenital heart failure that required palliation surgeries for survival. Since his heart transplantation (HTx) at 29 years, he has been able to very significantly improve his peak oxygen uptake (VO2peak), exercise capacity and quality of life. The evidence suggests that this will confer long-term clinical benefits.
An individualised exercise plan was designed and administered by an accredited exercise physiologist and enthusiastically embraced by the patient. His exceptional improvements in VO2peak and exercise capacity following HTx are well in excess of mostly modest or absent rises described in the literature.
Exercise training will continue to be important to limit the impact of immunosuppressive therapy on exercise capacity and quality of life.
Heart rate at rest and responses to exercise indicate that chronotropic competence has continued to develop over the first 2 years following HTx.
References
Footnotes
Contributors Roles of the authors in this case report. SS: clinical cardiovascular exercise physiologist who provided the exercise physiology services for the patient from 2009 to 2016 inclusive, and was responsible for obtaining the patient’s permission and the patient’s perspective. He also led the preparation of the first, subsequent and final drafts of the manuscript. He is the corresponding author. SF: clinical exercise physiologist who assisted with the exercise physiology services for the patient from 2015 to 2016, and contributed to all drafts of the manuscript. MJFH: clinical cardiovascular exercise physiologist and researcher who made significant contributions to formulating the main directions of the manuscript and reviewing and editing all drafts.
Funding Professor Haykowsky’s research is supported by the Moritz Chair in Geriatrics, College of Nursing and Health Innovation, University of Texas at Arlington.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.