Article Text

Summary
Budd-Chiari syndrome (BCS) is characterised by obstruction of hepatic venous outflow and may be triggered by the prothrombotic state associated with inflammatory bowel disease (IBD). We reported a case of Crohn’s disease (CD) that presented with anasarca, ascites, symptomatic hepatomegaly, elevated liver enzymes, increased prothrombin time and low albumin. Oesophagogastroduodenoscopy and colonoscopy confirmed active CD. Abdominal CT showed hepatic vein thrombosis. Liver biopsy revealed severe perivenular sinusoidal dilation with areas of hepatocyte dropout, bands of hepatocyte atrophy and centrizonal fibrosis, suggestive of BCS. The patient was treated with steroids for CD and systemic anticoagulants for BCS. His liver function and enzymes normalised, and he reported symptomatic improvement. The precise mechanism responsible for increased hypercoagulability in IBD remains unclear. Early recognition and treatment for possible thrombotic complications of CD is critical to prevent potentially fatal events like pulmonary embolism or liver failure.
- crohn’s disease
- liver disease
- pathology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Crohn’s disease (CD) is a type of inflammatory bowel disease (IBD) that can involve any part of the gastrointestinal tract. It causes a systemic inflammatory state that can involve the joints, eyes, liver, skin and haematological system. Generally, the systemic inflammatory response consists of fevers, chills, night sweats, myalgias and chronic fatigue. Elevation of acute phase reactants like the erythrocyte sedimentation rate and C reactive protein can also be observed. Common complications are gastrointestinal (GI) stricture and fistula formation, perforation, haemorrhage, malabsorption and hypercoagulability. The disease may induce a prothrombotic state leading to occlusion in both arteries and veins. Thrombosis have been reported to occur in hepatic veins, portal veins and in the inferior vena cava (IVC).1 Hepatic venous outflow obstruction is the underlying cause of Budd-Chiari syndrome (BCS), classically presenting with a clinical triad of abdominal pain, ascites and hepatomegaly. CD as a precipitant of BCS, although recognised, is extremely rare and there have been few reported cases.2–7 Here, we are presenting a unique case of BCS in a patient with CD who concomitantly developed hepatic vein and IVC thrombosis leading to the development of cirrhosis and showed substantial improvement with treatment.
Case presentation
A 27-year-old African-American man was admitted to our institution as a transfer from an outside hospital to receive a higher level of care due to new-onset ascites and bilateral lower extremity oedema for the previous 2 weeks. He had a history of intermittent abdominal pain, haematochezia and diarrhoea for the past year, when he was diagnosed with IBD at an outside hospital. At that time, he was prescribed mesalamine and steroids, which he took for a short period with improvement in his diarrhoea although he never achieved complete remission. Due to the cost of the medications, he discontinued them and was lost to follow-up for approximately 6 months. On admission, he complained of new onset of dyspnoea on exertion, fatigue and abdominal swelling. He had developed severe bloody diarrhoea over the last 1 month, suggestive of an acute flare in the setting of chronically uncontrolled disease. His physical examination revealed an alert and oriented individual with pale conjunctiva and no signs of icterus. He had prominent tachycardia (heart rate 124/min), bilateral pitting pedal oedema and a distended abdomen with the presence of shifting dullness, suggestive of ascites. The remainder of his physical examination was normal with no changes noted on the skin and he had intact arterial pulses in all four extremities.
Investigations
Laboratory studies determined that he had iron deficiency anaemia (haemoglobin 5.7 g/dL, mean corpuscular volume 57 fL, undetectable serum iron and ferritin of 9 mg/dL) from chronic gastrointestinal blood loss, normal bilirubin (total: 0.8 mg/dL and unconjugated: 0.4 mg/dL) and creatinine (0.6 mg/dL) levels, increased prothrombin time (16.6 s), hypoalbuminaemia (2.2 g/dL) and elevated liver enzymes (alkaline phosphatase: 138 U/L; alanine transaminase: 83 U/L; aspartate transaminase: 81 U/L). Stool examination revealed positive faecal leucocytes but was otherwise negative for faecal culture for enteric pathogens including Clostridium difficile toxin, Giardia antigen, Cryptosporidium antigen and other ova and parasites. The elevation of his liver enzymes remained unexplained, as he had no history of alcohol abuse and serological studies for hepatotropic viruses were negative. Laboratory studies performed to evaluate for Wilson’s disease, alpha-1 antitrypsin deficiency, autoimmune hepatitis, non-alcoholic steatohepatitis and primary biliary cholangitis were also negative.
Abdominal ultrasound showed hepatomegaly with moderate ascites. Ascitic fluid was sampled which showed <250 neutrophils and serum ascites albumin gradient of >1.1 consistent with portal hypertension. Oesophagogastroduodenoscopy and colonoscopy to further evaluate his bleeding and history of IBD were performed. Oesophagogastroduodenoscopy revealed erythema in the antrum of stomach and multiple superficial duodenal ulcers (figure 1). Biopsies from the upper and lower GI tract showed gastroduodenitis, a granuloma in the stomach (figure 2) and terminal ileitis. Colonoscopy revealed prominent ulceration in terminal ileum and caecum with few areas of erythema in the rest of colon. Based on these features, including the endoscopic appearance and histology findings, a diagnosis of CD was made. He underwent abdominal CT scan, which showed evidence of thrombi in the hepatic vein, IVC and portal vein; hepatomegaly with areas of liver injury and relative sparing of caudate lobe and large volume ascites (figure 3). A transcutaneous liver biopsy was obtained which showed stage 4, primarily centrizonal fibrosis, with partially obliterated central veins, areas of hepatocyte dropout and clusters of perivenular haemosiderin-laden macrophages (figure 4). The histopathological features were consistent with hepatic cirrhosis due to BCS. Except for the liver fibrosis, no other extraintestinal manifestations of CD were present.

Endoscopic image of second portion of duodenum showing multiple superficial ulcers with mucosal erythema.

(A) Gastric mucosal biopsy showing non-necrotising granulomatous lymphocytic inflammation in a background of chronic active gastritis, consistent with the patient’s diagnosis of Crohn’s disease (CD) (H&E stain, ×20 magnification). (B) Duodenal biopsies showing extensive neutrophilic and lymphocytic inflammation extending beyond the muscularis mucosa, consistent with the patient’s diagnosis of CD (H&E stain, ×20 magnification). The terminal ileum and colon also showed patchy areas of cryptitis, architectural distortion and granulation tissue (images not shown).
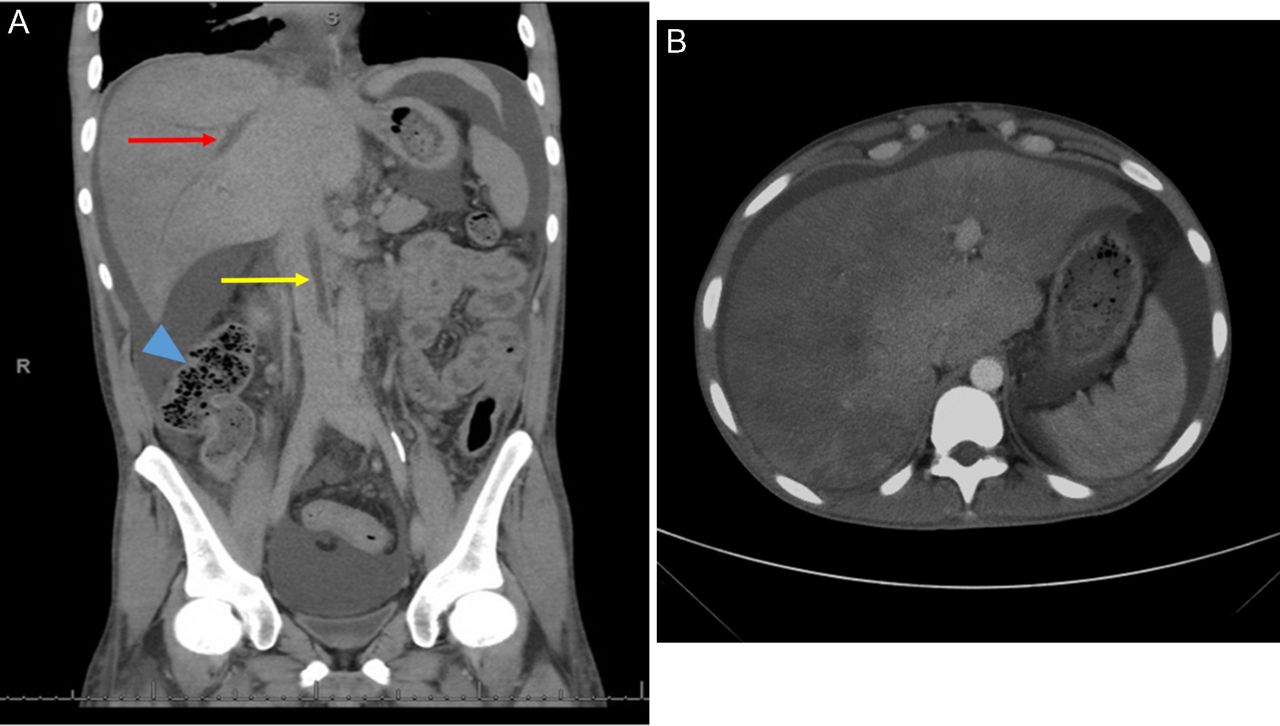
CT scan of abdomen and pelvis. (A) Coronal view showing thrombosis in the common hepatic vein (red arrow) and a partially occluding thrombus in the inferior vena cava (yellow arrow). The diseased ileum in the lower abdominal quadrant is marked with an arrow head. (B) Transverse view showing diffuse hepatic parenchymal injury with sparing of the caudate lobe.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
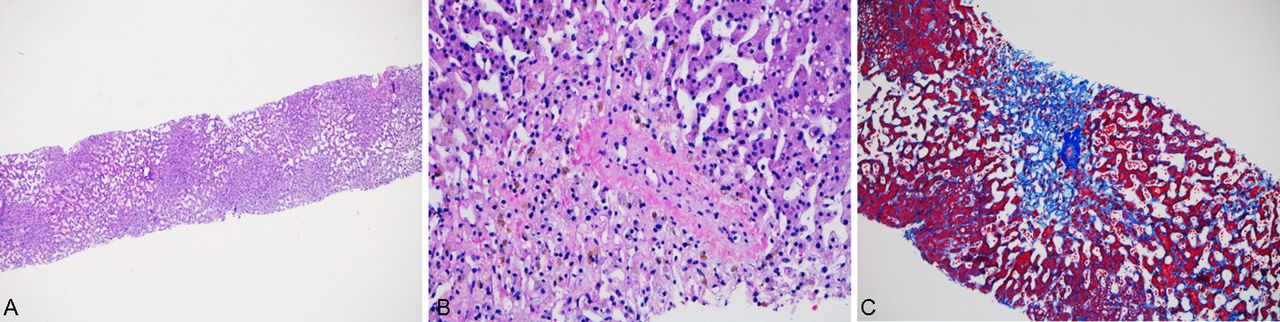
(A) The patient’s liver biopsy showed extensive perivenular sinusoidal dilation, bands of hepatocyte atrophy, haemosiderin deposition (primarily within macrophages; (B)), areas of hepatocyte dropout and occasional occlusion of central veins (B, arrow). (C) A Masson’s trichrome stain showed central veins (arrow) with prominent centrizonal fibrosis, diffuse subsinusoidal fibrosis and areas of bridging.
Treatment
The patient was transfused with packed red blood cells for his symptomatic anaemia and started on oral prednisone and a low dose of 20 mg intravenous furosemide every 12 hours for 2 days followed by oral spironolactone and furosemide for his CD and anasarca, respectively. To prevent detrimental changes in osmolality, no albumin infusion was given to the patient, since he had already received multiple packed red blood cell transfusions which raises serum osmolality.
He was also started on heparin intravenous infusion and then transitioned to oral apixaban for long-term anticoagulation therapy. He was not evaluated for an underlying hypercoagulable state during his illness due to financial constraints and his uninsured status.
Outcome and follow-up
Eventually the patient’s clinical status improved and he was discharged. He was followed up in clinic and was started on azathioprine and sulfasalazine with a plan to slowly taper his steroids. This was followed by initiation of adalimumab therapy. During his sequential follow-up visits, his abdominal pain improved, GI bleeding was absent, bowel movements were reduced to about two per day, he gained 10 kg of weight, lower extremity swelling resolved and abdominal distension nearly normalised.
Discussion
The incidence of IBD has increased dramatically during the last four decades, with approximately 5 million individuals affected in North America and Europe.8 Although IBD primarily affects the bowel, there are many known secondary effects on patients with IBD that are now widely accepted, including an increased risk of venous thromboembolic events, liver disease, cancer and bone disease.8–10 Thrombosis in IBD is characterised by both systemic venous thromboembolic events and focal microthrombi in the vasculature of the inflamed intestine.11 There are several proposed aetiologies for this increased risk, including thrombocytosis and platelet activation,12 hyperhomocysteinaemia,13 increased fibrinogen,14 impaired fibrinolysis,15 autoantibodies,16 17 elevated procoagulation factors and/or decreased anticoagulation factors18 19 and procoagulation mutations,20 yet no consensus has emerged.8 10 11
The portal venous system drains blood to the liver from majority of the gastrointestinal tract (except the anus), spleen, pancreas and gall bladder. The superior and inferior mesenteric veins join the splenic vein to form the portal vein which carries blood to the liver. The blood from the liver is drained by the hepatic veins into the IVC. BCS can be characterised as any pathophysiological process that results in interruption or diminution of the normal blood flow out of the liver, either within the hepatic veins or IVC. The occlusion in the extrahepatic venous system may on occasion, cause portal vein thrombosis. There is considerable overlap in the aetiology and clinical management of patients with BCS and portal vein thrombosis. Venous obstruction in the liver is distributed in the following frequencies of incidence: 62% in the hepatic veins, 7% in the IVC, 31% involving both and 14% within the portal vein.1 Symptomatic patients with BCS typically present with ascites, abdominal pain, hepatomegaly and in some cases hepatic necrosis leading to acute liver failure. BCS leads to hepatic congestion, portal hypertension, ascites, oesophageal varices and eventually cirrhosis. It can be classified as acute, subacute or chronic. An underlying disorder can be identified in over 80% of cases, with myeloproliferative disorder being the most common cause of acquired BCS.21 22 The underlying aetiology may be acquired or inherited; the most common have been listed in box.23
Most common causes of acquired and causes of inherited thrombophilia implicated in Budd-Chiari syndrome and portal vein thrombosis23
Acquired
Chronic myeloproliferative disorders.
Inflammatory bowel disease.
Oral contraceptives.
Antiphospholipid antibodies.
Pregnancy.
Polycythaemia vera.
Bacterial and fungal infection.
Essential thrombocytopenia.
Tumours.
Inherited
Factor V Leiden mutation.
Prothrombin G20210A mutation.
Antithrombin deficiency.
Protein C deficiency.
Protein S deficiency.
The risk of developing BCS in patients with CD is higher during IBD ‘flares’.24 Individuals with IBD have a threefold to fourfold increased risk of developing venous thromboembolic events.9 Notably, several studies have demonstrated that proinflammatory cytokines can counteract natural anticoagulant activity leading to a hypercoagulable state.17 18 The diagnosis of CD usually precedes or occurs simultaneously with the diagnosis of BCS.24
In our patient, CD was diagnosed more than 1 year before the diagnosis of BCS. CD can lead to thrombosis of critical areas like the dural venous system in the brain or the pulmonary vasculature, which can lead to life-threatening outcomes.4 5 Furthermore, hepatic venous outflow obstruction in BCS can lead to severe liver failure; without treatment, severe congestion and necrosis lead to fibrosis and ultimately cirrhosis.25 26 In some patients, liver function deteriorates so rapidly that they present with acute liver failure.
Due to the various clinical manifestations of BCS, an early histological evaluation to determine severity of the hepatocellular damage is usually recommended, but its role in management and prediction of outcome remains controversial.27 Histologically, BCS can present with centrilobular congestion, centrilobular necrosis, lobular inflammation, portal inflammation, pericentral fibrosis, periportal fibrosis and/or cirrhosis in the most severe cases. Our patient’s liver biopsy revealed severe perivenular sinusoidal dilation with areas of confluent hepatocyte dropout, bands of hepatocyte atrophy and centrizonal fibrosis, consistent with chronic outflow obstruction/BCS (figure 4).
One study proposed a histology-based algorithm for the treatment of BCS, suggesting that patients with BCS should be treated solely with oral anticoagulants when the biopsy reveals only central lobular venous congestion with sinusoidal dilatation.28 In cases where pericentral necrosis is present, a decompressive shunt procedure (like transjugular intrahepatic portosystemic shunt) is recommended, while liver transplantation is recommended in presence of extensive fibrosis. Individuals with IBD after an initial episode of venous thromboembolic events are at increased risk of developing another episode after discontinuation of anticoagulation therapy.9
Our patient has been kept on anticoagulation therapy and no further episodes of thrombosis have occurred. BCS is a rare complication of CD and when left untreated can cause significant liver damage and can lead to death. This case recapitulates the need for a high level of suspicion and increased awareness of the venous thromboembolic risks associated with CD. Radiological imaging coupled with histological diagnosis plays an important role in early detection and assessment of the extent of disease in BCS. Appropriate intervention to mitigate hepatic congestion is essential to restore hepatic function and to alleviate portal hypertension.
Learning points
The prothrombotic state in inflammatory bowel disease may lead to thrombosis in hepatic veins leading to Budd-Chiari syndrome (BCS) and/or thrombosis in portal veins resulting in portal hypertension.
In the presence of liver function test abnormalities, abdominal imaging should be performed to evaluate for BCS, among others.
BCS may be associated with Crohn’s disease and although no clear mechanism has been described, it is suspected to be multifactorial.
Early recognition and treatment of BCS with systemic anticoagulants can prevent a fatal outcome, such as pulmonary embolism or liver failure, and may reverse hepatic functional abnormalities (eg, hypoalbuminaemia and increased prothrombin time), as observed in our patient.
References
Footnotes
CCS and YAG contributed equally.
Contributors YAG and SNM are the physicians who evaluated and treated the patient. YAG and CCS formulated the initial draft of the manuscript. HLS made the diagnosis of Budd-Chiari on the liver biopsy, edited the manuscript and directed the overall project.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.