Article Text

Statistics from Altmetric.com
Description
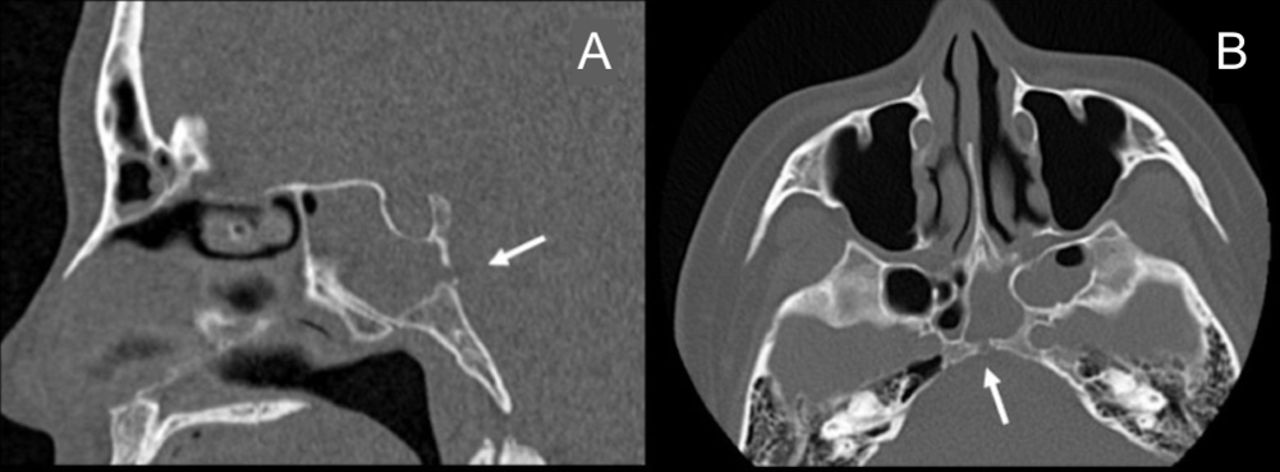
A 41-year-old woman with 7 days of fever and headache had loss of consciousness 1 day prior to presentation. Despite the absence of trauma or other significant medical history, she had two episodes of meningitis in the previous 6 months. Physical examination showed no nuchal rigidity or abnormal findings on nasal endoscopy. Lumbar puncture showed a cerebrospinal fluid cell count of 750/μl. CT showed a bony defect of the posterior wall of the sphenoid sinus, which was filled with a soft tissue density. MRI showed fluid intensity in the same area (figure 1A, B). The diagnosis was recurrent meningitis due to possible idiopathic cerebrospinal fluid rhinorrhoea. Although a cisternogram is normally recommended, emergency drainage of the sphenoid sinus with antibiotic treatment was prioritised because of her deteriorating condition. With various possible diagnoses, an experienced surgeon operated on the patient.

{kind=link}
A bony defect of the posterior wall of the sphenoid sinus (arrows): (A) CT with sagittal view and (B) CT with axial view.
Endoscopic sinus surgery was performed emergently under general anaesthesia for drainage and reconstruction of the bony defect, 6mm below the sella floor (online supplementary video 1) in the sphenoid sinus.
Supplementary file 1
The exact site of the submucosal defect was identified and reconstructed with nasoseptal mucosal flap with fat (online supplementary video 2) watery rhinorrhoea stopped soon after the operation. She was treated with cefotaxime 6 g/day for 2 weeks, made good progress and was discharged. At 38 months postoperatively, there is no evidence of recurrence based on both endoscopic evaluation and radiographic analysis.
Supplementary file 2
Learning points
Idiopathic cerebrospinal fluid rhinorrhoea (ICFR) is seen most often among middle-aged obese women. These patients tend to experience rhinorrhoea as the primary symptom, but meningitis is also often an initial symptom.
The typical cause of ICFR in the sphenoid sinus appears to involve a congenital bone union disorder of the posterior and lateral walls of the sinus, sometimes with meningoencephalocele. CT in this case showed a bony defect on the posterior wall of the sphenoid sinus, 6 mm below the sella floor. The exact site of the submucosal defect must be identified to achieve close approximation for reconstruction with abdominal fat, and sometimes a nasoseptal mucosal flap.
In cases of recurrent meningitis with cerebrospinal fluid rhinorrhoea, transnasal reconstruction with endoscopic sinus surgery is the first choice. Early consultation with otolaryngology and surgical reconstruction lead to a good outcome.
Footnotes
Contributors MH and KO experienced this case. MH drafted the manuscript, and KO designed the figures and videos and did critical revision of the article. NO and YT gave final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.