Article Text

Summary
February is a busy month for the ambulance skiing patrol at the skiing resorts in Norway and on this day, a call regarding an 11-year-old boy on one of the hills reached the team. What no one knew at that moment was that this boy had suffered a unique injury and that his X-rays would reveal something that, prior to this, had never been described in the history of mankind. This patient had suffered a simultaneous avulsion fracture of both the femoral and tibial insertion sites of the anterior cruciate ligament without suffering any other injuries to the knee. The injury was treated conservatively and at 1-year follow-up, the patient was completely recovered.
- paediatrics
- orthopaedics
- knee injuries
- ligament rupture
- knee laxity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Ruptures of the anterior cruciate ligament (ACL) are common orthopaedic injuries, especially among patients participating in pivoting sports. The mechanism of injury is often similarly described in the paediatric population. However, in the skeletally immature patient, the ACL withstands higher forces than the incompletely ossified insertion sites of the ligament.1 As a result, the trauma may spare the ACL from rupture and, instead, an avulsion fracture of the bony insertion sites of the ligament may occur. The ACL originates at the posteromedial aspect of the lateral femoral condyle and inserts anteriorly on the medial tibial intercondylar eminence. Although avulsion fractures of both the proximal and distal insertion sites have been described, the tibial eminence fracture is by far the most commonly occurring of the two, predominantly affecting children aged 8–14 years.1–4 The incidence of the tibial eminence fracture is, however, low, with numbers of approximately three per 100 000 per year.5 For this reason, the hospital employees who encountered the patient described in this case report were experiencing something extremely rare, when a young boy suffered an injury involving both the femoral and the tibial attachments of the ACL.
Case presentation
This boy was a healthy, active 11-year-old who played soccer in his spare time. He and his father were enjoying downhill skiing at a resort in Norway, when another skier, travelling faster, suddenly approached and the collision was unavoidable. The boy was hit on the lateral aspect of his right knee with his foot planted on the ground. This resulted in a pivoting movement with knee valgus and external tibial rotation. The patient was initially cared for at a local hospital, close to the resort. On first examination, he was unable to extend his knee fully and had a knee flexion of about 70°. The patellar apprehension test was negative, he had no pain when palpating the tibiofemoral joint line and he was stable to valgus and varus stress. Plain radiographs showed that the boy had suffered a tibial eminence fracture (figure 1). However, what particularly caught the radiologist’s attention was a bony avulsion fragment of uncertain origin. It was assumed to originate from the tibial side, since no femoral defect could be seen. The patient was given a temporary high leg cast and was transferred to another hospital for inpatient care and an MRI evaluation.

Frontal plain radiograph of the right knee showing the medial intercondylar avulsion and the femoral avulsion.
The MRI confirmed the medial intercondylar avulsion fracture of the tibia but dismissed the initial thought regarding the origin of the other fragment. This fragment was instead described as ‘a skull-shaped fragment corresponding to the ACL origin of the medial aspect of the lateral femoral condyle’. An additional CT was performed to further assess the pathology of the proximal bony fragment and the interpretation was identical (figures 2A,B and 3A,B). So, this patient had suffered a simultaneous avulsion fracture of both the proximal and distal insertion sites of the ACL.

CT images of the fractures. (A) Coronary view indicating both the femoral and the tibial avulsion fractures. (B) The femoral avulsion fracture visualised at the medial aspect of the lateral condyle.
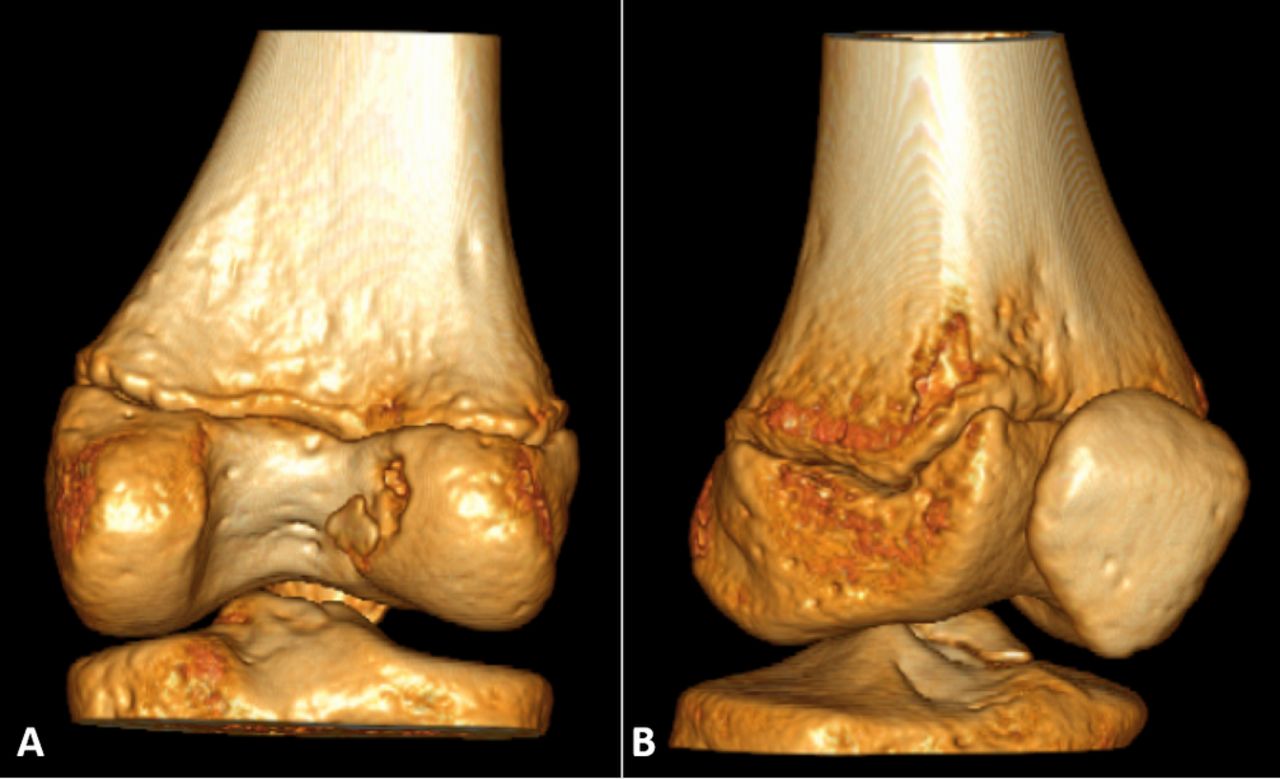
(A) Three-dimensional CT image from a posterior view indicating the femoral avulsion. (B) Anterolateral view enables visualisation of the tibial avulsion fracture.
Treatment
Conservative treatment was decided on in this unusual case, with a knee brace locked in full extension for 4 weeks. When 4 weeks had elapsed, the CT scan showed that the fragments were still in their original position, but the fractures were still highly visible. It was, therefore, decided to extend the treatment period with a brace to a total of 6 weeks.
Outcome and follow-up
When the patient returned 12 weeks after the injury, he was able to walk without a limp and did not describe any severe problems with his knee. The MRI showed signs of healing for both fragments and an intact ACL. However, the Lachman examination of the involved knee was interpreted as a 2+ without a secure end point and the boy was assigned to an enhanced rehabilitation programme. At the final follow-up, a year after injury, another MRI was completed. With the exception of minimal oedema around the tibial insertion site of the ACL, no pathology could be visualised. The fracture line at the eminentia intercondylaris could barely be distinguished and, when it came to the femoral origin, there was no sign of injury (figures 4–6). The knee examination was perfectly normal with symmetric knee range of motion and thigh circumferential of the involved leg compared with the non-involved one. A firm end point could be distinguished when performing the Lachman examination and the patient himself felt that he had completely recovered, without any perception of instability.

Sagittal projection of the MRI at 1-year follow-up.

Frontal projection of the MRI at 1-year follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coronal-oblique projection of the MRI at 1-year follow-up.
Discussion
Although ACL insufficiency in children is rare, avulsion fractures of the tibial insertion site alone and its management are well recognised. However, only a few cases of avulsion fractures involving the femoral insertion site have been described in the literature6–13 and the first detailed description of a patient undergoing arthroscopic repair of an injury of this kind was published as late as 2006.9 The case presented here represents an extreme rarity and, to our knowledge, a similar injury, affecting both insertion sites, has only been described once before.14 However, there is also diversity between these cases, making the current case totally unique. The historically similar case was presented about four decades ago and involved a 13-year-old boy who sustained a twisting injury to his knee when falling from a motorbike. He presented with a moderately swollen knee and complained of pain. However, instability caused by ACL insufficiency was only evident on physical examination under anaesthesia and muscle relaxation, implying a positive anterior drawer sign (2+). Moreover, this boy demonstrated gross medial laxity which corresponded to a simultaneous injury to the medial collateral ligament of the knee.14
It is only possible to speculate about how the mechanism of injury might differ between single avulsion fractures of the ACL and those involving both insertion sites. The authors presenting the previous case hypothesised that the fracture of the tibial eminence was the result of a blow from the femoral condyle in response to the tibial rotation, while, in the meantime, tensile forces were transmitted in a proximal direction and thereby caused a concurrent fracture of the femoral insertion.14 Although there are several similarities between the two cases, our patient had no associated injuries and no significant displacement of the fractures, different from the first case. It is therefore likely that the trauma and the forces applied to the knee were more severe in the previous case and it therefore appears that no associations between the impact of the magnitude of forces and the risk of simultaneous avulsion fractures could be identified. Given the fact that no concomitant injuries occurred in our patient, it is reasonable to assume that a force was strictly applied to the ACL at the moment of injury. The combination of an axial vector in the direction of the ACL with an instantaneous and concurrent avulsion at both insertion sites would theoretically swiftly reduce the traction forces, thereby constraining the displacement of the fragments, as observed in this patient.
A radiological evaluation is essential when assessing the diagnosis and plain radiographs are the preferable first-line approach in the clinical setting. As different from our patient, in whom both fragments were detected on the regular anteroposterior and lateral X-rays, the femoral avulsion could only be visualised on a notch/tunnel roentgenogram in the previous case.14 It is noteworthy that this radiographic view is not always considered as a matter of routine. Furthermore, it must be emphasised that the slit fragments in the youngest patients could be purely cartilaginous, thereby requiring MRI for detection.15 16 These circumstances underline the importance of performing a thorough investigation in order to rule out any possibilities of concurrent femoral involvement when establishing the diagnosis of a tibial eminence fracture in children.
The tibial eminence fracture has been historically classified according to Meyer and McKeever17 and it was subsequently updated according to Zaricznyj.18 This classification is divided into four grades; no displacement (type I), displacement and hinging of the anterior third or half of the eminence (type II) and complete displacement of an intact fragment (type III) or a comminuted fragment (type IV). Type I fractures can be treated conservatively, while the others require surgical intervention.2 15 In this case, conservative treatment was chosen, since neither the tibial nor the femoral fracture was significantly displaced. The boy showed excellent recovery at the final follow-up and the prognosis was deemed good, without any particular concerns about future deficiency. It has been reported that the ACL could still have been stretched beyond its physiological properties at the time of injury, although no evident rupture of the ligament could be seen,19 which could possibly cause persistent instability, even if the fracture healed well. A recent study showed that approximately one-fifth of patients required a delayed ACL reconstruction after suffering a tibial eminence fracture.19 Similarly, a meta-analysis of studies reporting the incidence of residual laxity following tibial eminence fractures revealed that approximately one-fifth of patients with types I and II fractures had a positive Lachman test after treatment. However, a positive Lachman test was three times more frequent in patients with types III or IV fractures, where the majority reported having a positive test.2 These findings underscore the importance of a correct diagnosis, treatment and follow-up of young patients presenting with a suspected injury to the ACL or its insertion sites. Knowledge of unique cases could potentially enhance awareness when detecting variable injury patterns and optimise treatment based on each individual case.
Learning points
Knee joint trauma in children should always be investigated thoroughly.
The radiological evaluation should be performed with the awareness of a possible concurrent femoral avulsion fracture in addition to the tibial eminence fracture.
Non-displaced avulsion fractures have the potential to heal successfully when conservatively treatment is chosen, however, a proper clinical follow-up is necessary to ascertain a satisfactory knee function in both the short-term and the long-term perspective.
References
Footnotes
Contributors KS, ES, EHS and BO have substantially contributed to the writing of this manuscript and are responsible for drafting the work and revising it critically for important intellectual content. All authors have given their final approval of the manuscript to be published.
Competing interests None declared.
Patient consent Guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.