Article Text

Summary
We report a novel electroconvulsive therapy (ECT) regimen for sustaining the resolution of behavioural and psychological symptoms of dementia (BPSD) using alternating acute and maintenance ECT (M-ECT) trials. A 64-year-old man presenting with major neurocognitive disorder was admitted for acute behavioural disturbances and physical aggression. With few treatment options, the impact on patients’ quality of life often supersedes cognitive symptoms and is a predictor of long-term institutionalisation. Recent studies indicate that ECT may be an effective and safe way to address BPSD. Clinicians have little information about when and how to stop a successful course of acute ECT or the long-term advantages of M-ECT with subsequent intermittent acute ECT. This case emphasises the benefit of M-ECT and describes potential challenges associated with abrupt discontinuation. This case is the first to detail tapering ECT for treatment of aggression in dementia by interchanging acute and M-ECT courses in response to symptom burden.
- geriatric medicine
- medical management
- memory disorders (psychiatry)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Major neurocognitive disorders (MNDs) may give rise to non-cognitive behavioural and psychological symptoms of dementia (BPSD), a syndrome characterised by physical and verbal symptoms, both aggressive and non-aggressive.1 Fifty to ninety per cent of patients diagnosed with MND experience BPSD.2 3 Agitation and aggression, often the most disruptive of these behavioural complications, result in severe adverse effects on MND patients quality of life and is a risk factor for long-term institutionalisation and increased use of psychotropic medications.1 4 5 The behaviours are often modestly managed using antipsychotics, which are associated with dangerous side effects and increased risk of mortality.6
There is growing evidence that electroconvulsive therapy (ECT) can safely and effectively treat behavioural symptoms of dementia when treatment regimens have been exhausted or proven ineffective.7 8 Rates of relapse postacute ECT are as high as 80% within the first 6 months of discontinuation among patients with major depression,9 suggesting there may be ramifications to discontinuing ECT shortly after symptoms improve. While continuing postacute treatment may sustain improvements in BPSD, there is an absence of findings on the rates of relapse post-ECT treatment. Seven case reports,10–16 one chart review of 16 patients,7 one cohort study of 8 patients and a naturalistic prospective study of 23 subjects,17 18 discuss the management of acute ECT for severe aggression and agitation among patients with MND; however, the findings do not provide guidance for maintaining remission, including the tapering or discontinuing of ECT. Geriatric depression literature and clinical experience remain the only resources available to maintain a successful course of ECT for BPSD and make long-term treatment recommendations for sustaining improvements. Therefore, we report a unique case of ECT management for MND to demonstrate an effective example of alternating the administration of acute and long-term maintenance ECT (M-ECT) trials to sustain improvements in agitation and aggression in a patient with severe BPSD.
Case presentation
A 64-year-old man, with a progressive cognitive and functional decline over a 5-year period and an acute exacerbation of behavioural symptoms was discharged from a long-term care facility and admitted to an acute care hospital. After 9 months in long-term care and worsening symptoms, he was transferred to a geriatric mental health inpatient unit for assessment and treatment. His acute change in behaviour consisted of inappropriate sexual behaviour, stimulus-bound behaviours, aberrant motor behaviours, aggression to people and property and intrusiveness. He often required seclusion and pharmacological restraints to reduce the risk of harm to others.
His medical history includes long-standing bilateral deafness, a history of hypertension and a recent history of pneumonia. Physical and neurological examinations, first completed by a geriatrician in the acute care hospital and second completed by the geriatric inpatient unit hospital, revealed no significant medical or neurological findings, specifically gait abnormalities and parkinsonism. The patient was able to live on his own, attained secondary-level education, travelled and held employment in low-skill administration for 20 years prior to his decline. One health record from a previous institution noted a possible diagnosis of schizophrenia. He denied psychotic symptoms, and there was no evidence of responding to internal stimuli. After consulting with the patient and speaking with family, the clinical team could not corroborate this diagnosis. Following admission to the geriatric mental health inpatient unit, no symptoms of schizophrenia were observed over the patient’s first 2 years of institutionalisation and oversight by the clinical team. Further, there was no evidence of past psychotic symptoms, mood symptoms, treatment with antipsychotics or previous psychiatric admissions. Prior to admission, the patient was treated with escitalopram 15 mg/day and donepezil 10 mg/day. The duration of these trials were not included in the patient’s record.
Investigations
On arrival, the patient could not complete cognitive tests due to the severity of his aggressive behaviour. At baseline, the patient scored 0 out of 30 (norm for age and education level is 28)19 on the Mini-Mental State Exam (MMSE).20 On the Neuropsychiatric Inventory Clinician (NPI-C),21 he scored 72 out of 144 (figures 1 and 2).

NPI-C 12-item version was used to calculate total NPI scores over the duration of ECT treatments. b.i.d., two times a day; ECT, electroconvulsive therapy; MMSE, Mini- Mental State Exam; NPI-C, Neuropsychiatric Inventory Clinician; q.i.d., four times a day; t.i.d., three times a day.

Agitation, aggression, disinhibition and aberrant motor disturbance were scored using the NPI-C 14-item version over the duration of ECT treatment. ECT, electroconvulsive therapy; NPI-C, Neuropsychiatric Inventory Clinician.
The patient did not endorse any depression symptoms that fulfil the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition text revision (DSM-V-TR) criterion for depressive disorders. On the Cornell Scale for Depression in Dementia, the patient scored 4, indicating the absence of significant depressive symptoms.22
Laboratory work investigations confirmed that other illnesses were not contributing to the patient’s current state. His thyroid-stimulating hormone level was slightly elevated at 4.60. A toxicology urine screen did not reveal any drugs of abuse. The patient was unable to attend an MRI scan due to agitation; however, a CT scan was within normal limits and did not show any evidence of cerebrovascular disease or focal atrophy.
Differential diagnosis
Following patient assessment and in conjunction with collateral from his family, a diagnosis of major neurocognitive disorders due to possible frontolobar degeneration, consistent with DSM-V criteria, was made. The patient presented with an insidious onset and gradual progression of cognitive and functional deficits, namely in social cognition and executive abilities including early behavioural disinhibition, loss of empathy and preservative behaviours. He did not present with any neurological signs and the diagnosis was based on clinical history and presentation. Imaging could not be completed due to the patient’s level of agitation that caused challenges for completing the investigations.
Treatment
On admission, the patient was placed on involuntary status due to the potential of causing harm to others, required one-to-one clinical monitoring and was placed in an intensive observation unit (please see figure 3 for timeline). He was initially treated with amlodipine 5 mg/day, vitamin B121000 µg/day, irbesartan 150 mg/day, lorazepam 1 mg three times a day, lurasidone 40 mg two times a day and memantine 10 mg two times a day. Trazodone, methotrimeprazine and lorazepam were administered only when needed for agitation (figure 4). Methotrimeprazine, similarly to other antipsychotics, has been proven effective in addressing neuropsychiatric symptoms of dementia.23
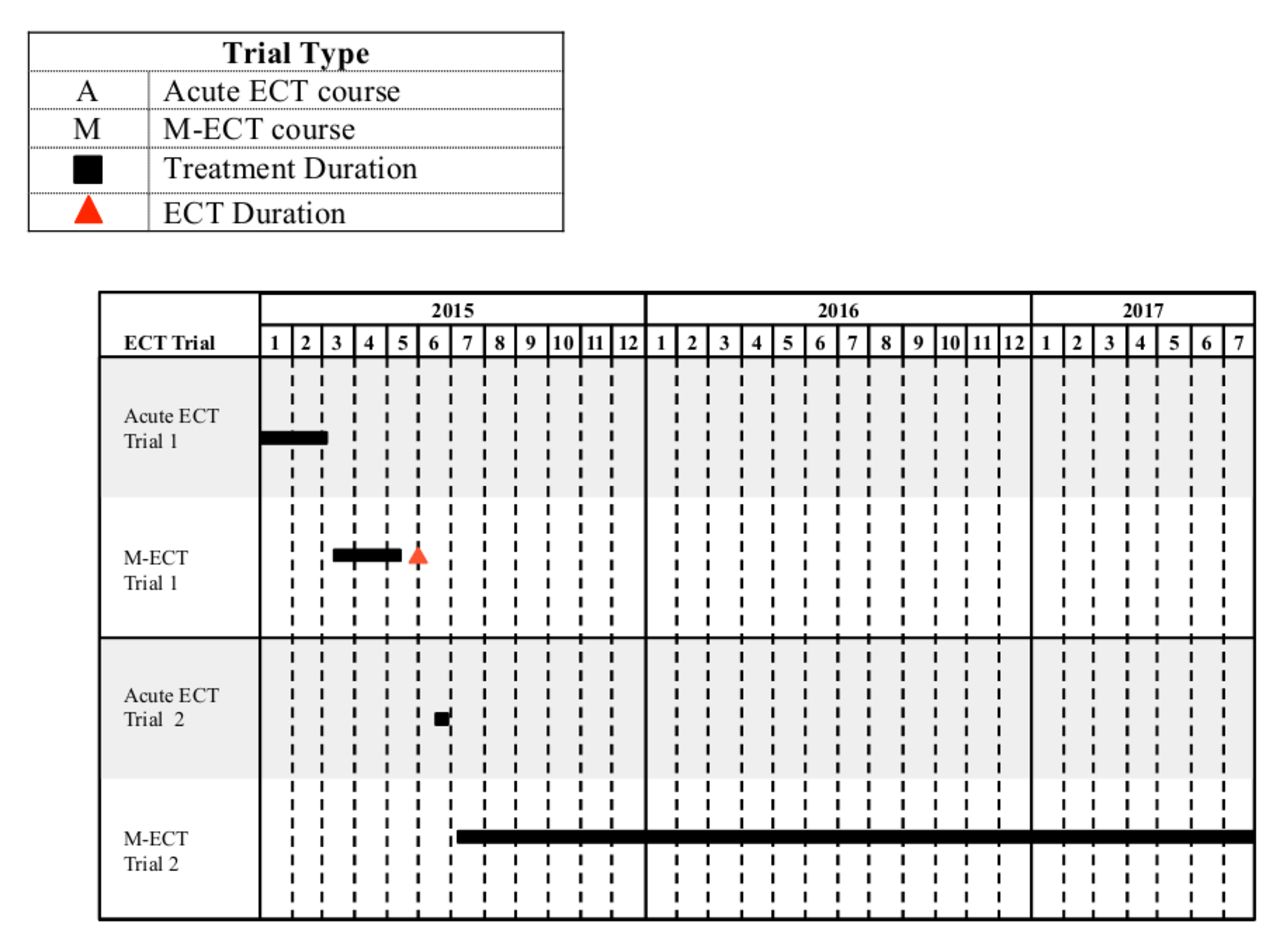
The course of acute ECT had to be discontinued because the patient developed pneumonia, resulting in an unintended additional 3-week gap between two treatments. ECT, electroconvulsive therapy; M-ECT, maintenance electroconvulsive therapy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multiple medications were trialled sequentially over the patient’s admission and either discontinued due to lack of significant benefit and adverse effects or maintained due to partial benefit. b.i.d., two times a day; ECT, electroconvulsive therapy; M-ECT, maintenance electroconvulsive therapy; q.i.d., four times a day; t.i.d., three times a day.
The patient was maintained on one-to-one clinical monitoring for the first 7 months of his admission due to the risk of harm to others. The patient’s state worsened during the later months of intensive monitoring, requiring seclusion up to five times a month. To improve BPSD symptom management, the patient was subsequently transferred to an intensive monitoring unit. Behaviours of grabbing tightly onto staff and copatients, intrusiveness, throwing objects, aberrant motor behaviours and voiding in inappropriate places continued. During the patient’s first 6 months of admission, multiple medications were trialled sequentially and either discontinued due to lack of significant benefit or adverse effects or maintained due to partial benefit (figure 4).
Behavioural interventions including exercise, music and engaging in activities were not effective. After 7 months and minimal success in addressing the patient’s BPSD symptoms through pharmacological and non-pharmacological strategies, an acute course of ECT was administered, consisting of two treatments per week. The patient was found incapable of making treatment decisions, and treatment was discussed with and consented by his family.
Bitemporal ECT was delivered using a MECTA SPECTRUM 5000Q ECT machine. Stimulus was titrated according to the clinical response at 1.5 times the seizure threshold to a max capacity of 576 millicoulombs (mC). At the first acute ECT session, the patient had a brief seizure lasting 13 s at 128 mC. The dose was increased to 192 mC at second treatment, reached 288 mC by the fourth treatment and was then further increased to 480 mC by the seventh treatment. Seizures were of borderline length. Due to lack of benefit, treatment was increased to the maximum dose of 576 mC by the eighth treatment.
During the first acute course of ECT, loxapine (20 mg three times a day) was added to the medication regimen and resulted in partial benefit with no side effects. After 15 treatments, the patient’s NPI score was a total of 8, with 0 in both agitation and aggression subscales (figures 1 and 2). MMSE scores were as high as 10. An M-ECT course was administered with the objectives of tapering treatment slowly to weekly and then biweekly. During the M-ECT course, the patient’s medication was minimised (figure 4).
Management of tapering procedure
The first M-ECT course began 8 days after the initial acute course ended and lasted for 2 weeks. The course had to be discontinued prematurely because the patient developed pneumonia, resulting in an unintended 3-week gap between two treatments. The pneumonia was not deemed secondary to the ECT and resolved within 2 weeks. His behaviours did not recur during this medical illness with an NPI ranging from 12 to 16, therefore, maintenance ECT was resumed at every 3 weeks from weekly with the hope that his BPSD would be stable. The patient’s symptoms of pneumonia were inconsistent with a comparable case assessing pneumonia as an underlying medical problem that had exacerbated agitation in a patient with severe BPSD.24 Unlike the comparable case, the patient’s BPSD symptoms worsened after pneumonia symptoms diminished.24 The patient’s symptoms returned 37 days from first M-ECT treatment. The patient’s NPI score returned to 72 and he required seclusion (figure 1). In response to worsened BPSD symptoms, practitioners began another acute ECT series at a frequency of two treatments per week at the maximum dose 576 mC for a total of nine treatments. By the fourth week of acute treatment, the patient had an NPI score of 31 (figure 1). The patient’s symptoms of agitation and aggression improved and he no longer required seclusion or one-on-one monitoring.
The second acute series was followed by a second M-ECT series, the frequency of which was tapered cautiously and conservatively. The course began with weekly treatment for 5 weeks. Treatment was then tapered to one treatment biweekly for 1 month, followed by one treatment every 3 weeks for 6 weeks. Treatment was then tapered to one treatment monthly. During this phase, the patient’s NPI score reduced to 22, and his MMSE had improved to 18 (figures 1 and 2). Quetiapine (50 mg nightly) was added to his pharmacotherapy regimen to aid sleep due to lack of benefit of other agents. Medroxyprogesterone was added during the second month of M-ECT and titrated to 50 mg two times a day over a 5-month period to address sexual disinhibition, which was a residual behaviour that did not respond fully to ECT. Behaviours associated with sexual disinhibition did not trigger seclusion or restraints.
Outcome and follow-up
M-ECT has continued for 17 months at a frequency of 1 ECT every 4 to 5 weeks. Targeted behaviours of agitation, aggression, motor disturbances and disinhibition remain improved. The patient no longer requires one-to-one support, his latest NPI scores are as low as 10, and he has had no adverse effects from the intervention (figures 1 and 2). The improved symptoms have sustained postdischarge and the patient is currently living in community-based long-term care. The patient currently receives M-ECT as an outpatient and exhibits no signs of deteriorating agitation and aggression.
Discussion
The current case report supports employment of alternating acute and maintenance ECT trials to treat patients with MND with severe and refractory BPSD. Acute treatment significantly reduced symptoms of agitation, aggression, motor disturbances and disinhibition, and response was sustained by a very slow tapering of M-ECT. This case offers post-ECT relapse prevention strategies in patients with severe and treatment-resistant BPSD, as well as methodologies for tapering ECT regimens in all populations.
Bilateral administration of ECT was well tolerated and did not cause side effects in this patient. Case reports and studies found no significant reduction in the patients’ abilities to execute instrumental and basic activities of daily living from baseline to discharge.11 15 18 The long-term impacts of ECT on cognition are unknown. Studies on younger cohorts suggest M-ECT does not result in adverse cognitive impairment (mean age 58.1 years old).25 In this case, bilateral ECT at maximum doses had a positive impact on cognition while stabilising behavioural disturbances. This is congruent with a study assessing the long-term cognitive function of geriatric patients after the administration of a large number of ECT treatments spaced over several courses.25 At present, this is one of few treatments to significantly improve both symptoms and cognition in this population. This study is the first to recommend tapering processes based on symptomatology in ECT for MND. Tapering methods from a randomised control trial using the Symptom-Titrated Algorithm-Based Longitudinal ECT algorithm for continuation ECT in prolonged remission in depressed elderly26 could be applicable to tapering ECT for MND.
There were medication changes that accompanied the ECT course; however, given the rampant worsening in behaviour when ECT was tapered too quickly, we believe ECT was the primary treatment leading to clinical improvement. This paper is the first to emphasise the benefits of tapering M-ECT instead of abrupt discontinuation in a patient who has experienced both alternatives, exemplifying the benefits of tapering M-ECT to sustain long-term symptom remission. This case report does not provide guidance on when M-ECT can be safely discontinued and further studies should explore this, given the difficulties accessing ECT and to ensure appropriate risk/benefit analysis of ongoing treatment.
Learning points
Alternating between acute and maintenance electroconvulsive therapy (M-ECT) dependent on patient symptomatology may be a good therapeutic option for treatment-resistant behavioural and psychological symptoms of dementia (BPSD) to sustain improvements in the long term.
Tapering ECT frequency slowly over several weeks to months can prevent relapse of BPSD.
Bilateral ECT can be well tolerated for a patient with a progressive major neurocognitive disorder.
Symptom burden should be measured in the long term to ensure effectiveness of M-ECT.
References
Footnotes
Contributors RW was chiefly overseeing the patient’s care. With this expertise, she led the analysis and preparation of the manuscript. Her role and leadership in electroconvulsive therapy regimens in the Canadian academic landscape enabled her to contribute to key messages in “Discussion” segment. OG and IF managed patient care, contributed substantially to the analysis and key messages of the paper and developed the manuscript. MIS provided support as a research student. Her key roles involved preparation of the manuscript, supporting the management of metrics, as well as collecting NPI-C and MMSE scores from clinical staff and patients.
Competing interests None declared.
Patient consent Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.