Article Text

Statistics from Altmetric.com
Description
A 57-year-old female presented with history of rapidly progressing multiple swellings over her face, forehead and sternum for the last 6 months (figure 1). On examination, these swellings were non-tender and hard in consistency. Her thyroid gland was not palpable. Thyroid function tests were normal. FNAC (Fine needle aspiration cytology) from the bony swelling revealed metastatic follicular thyroid carcinoma (FTC) (figure 2) with thyroglobulin (Tg) positivity on immunohistochemistry. Ultrasonography of the neck revealed a normal-sized thyroid gland with multiple hypoechoeic lesions and calcification. FDG-PET (Fluorodeoxyglucose - positron emission tomography) displayed diffuse osseous metastasis. She underwent total thyroidectomy, and histopathology was consistent with FTC. Postoperatively, serum Tg was 552 ng/mL (normal 1.4–78 ng/mL) and anti-Tg antibody was 15 IU/mL (normal <60 IU/mL). She also received zoledronic acid and high dose radioiodine ablation with scan showing a faint tracer uptake by the metastatic lesions. The patient was lost to follow-up and died a year after she presented first.

Clinical photograph of the patient showing multiple bony swellings over forehead, face and sternum.

{kind=link}
{kind=link}
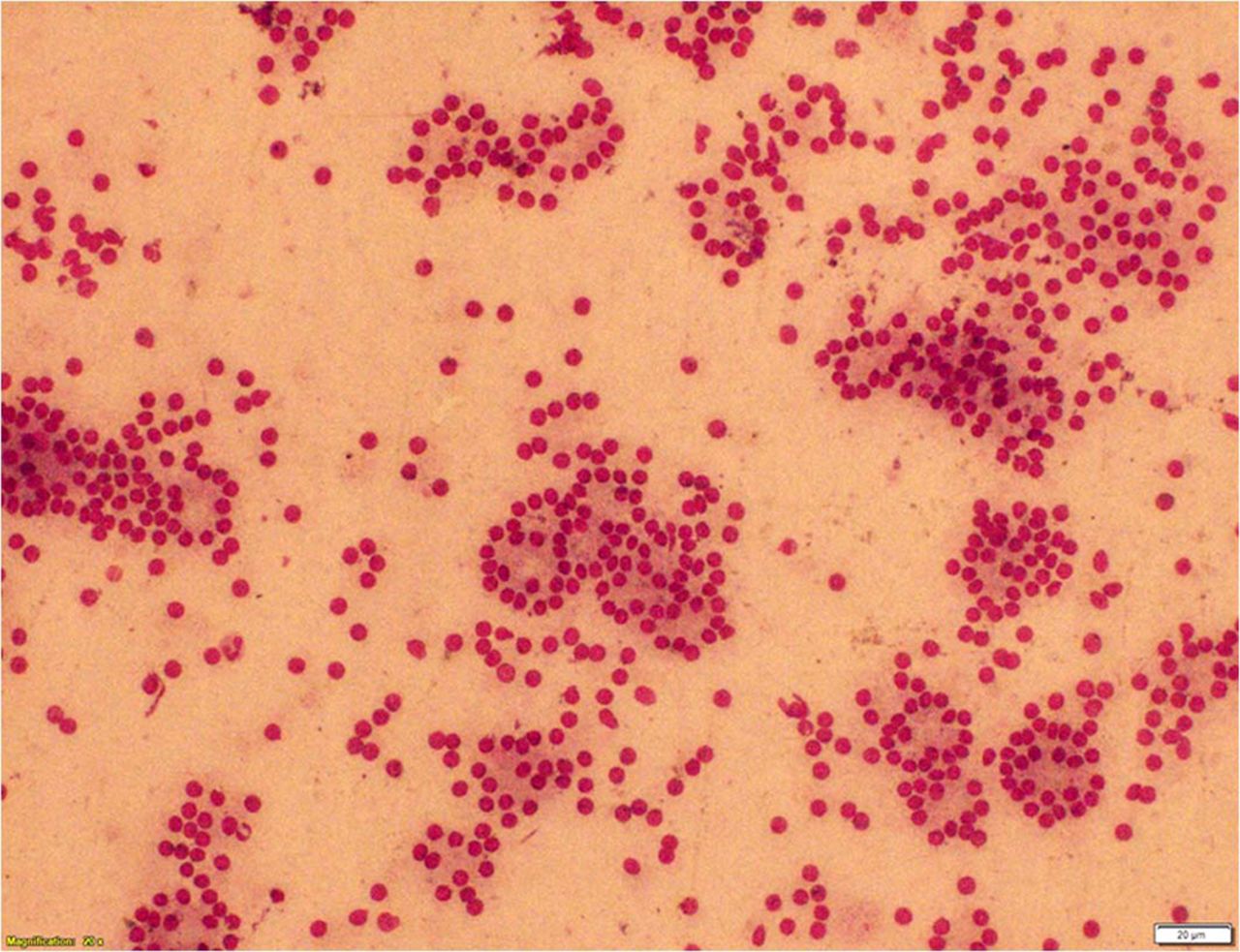
FNAC (Fine needle aspiration cytology) of the bony swelling showing abundant cellularity with cells showing predominantly follicular pattern.
Malignancies associated with a tendency to metastasize to flat bones include thyroid, breast and prostate carcinoma. Thyroid malignancy is rare and accounts for only 2% of all solid malignancies. FTC occurs in older people, the mean age at diagnosis being 50 years. Painless thyroid nodule is the most common presenting manifestation, while 1%–9% present with distant metastasis, as seen in our patient. The lung (50%) and bone (25%) are the most common sites of distant metastasis and bony lesions are mostly osteolytic.1 More than 80% of bone metastases from thyroid malignancies are located in the red marrow of the axial skeleton, where blood flow is high (eg, vertebrae, ribs and hips) and a conducive milieu exists for tumour growth due to the presence of growth factors, such as IGF-1 (Insulin-like growth factor-1) and IGF-2 (Insulin-like growth factor-2, FGFs (Fibroblast growth factors) and PDGFs (Platelet derived growth factors).2 Thyroid carcinoma with distant metastasis is associated with poor prognosis with 10-year survival rate of 40%.3
Learning points
Follicular thyroid carcinoma presenting with bony metastasis is quite uncommon.
Presence of bony metastasis in FTC is associated with poor prognosis.
Majority of the bony metastasis in FTC involve vertebrae, ribs and pelvic bones; however, skull involvement is not very frequent.
Lenvatinib, an oral multitargeted tyrosine kinase inhibitor, is an effective therapeutic alternative in radioiodine refractory metastases.
Footnotes
Contributors VSS prepared and edited the manuscript. AB diagnosed and managed the case and also edited the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.