Article Text

Summary
Posterior reversible encephalopathy syndrome (PRES) is a rare but well-described syndrome associated with a high morbidity and a substantial mortality. We present an illustrative case of an HIV-infected but virologically suppressed patient who complained of visual impairment accompanied by severe headache and epileptic seizures. The cerebral CT scan and the follow-up cranial MRI confirmed the diagnosis of PRES. Unlike the cases of HIV-infected patients with PRES published so far, our patient suffered neither from advanced immunodeficiency nor from opportunistic infection or from any other evident predisposing factor. This case highlights that the absence of classical risk factors does not exclude the diagnosis of PRES. We discuss the hypothesis that in accordance with the new pathophysiological theory, persistent HIV-associated cerebrovascular reactivity in combination with endothelial dysfunction may represent an undetected risk factor for the development of PRES in virologically and immunologically stable patients.
- hypertension
- HIV / AIDS
- epilepsy and seizures
- neuroimaging
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Posterior reversible encephalopathy syndrome (PRES), also known as reversible posterior leukoencephalopathy syndrome, is a spontaneously resolving syndrome characterised by the radiographic finding of a bilateral subcortical vasogenic oedema.1 The vasogenic oedema of the brain—predominantly involving the posterior parietal and occipital lobes2 3—is caused by an autoregulatory dysfunction of brain vessels. This leads to arteriolar dilatation and hyperperfusion together with hydrostatic leakage and interstitial fluid accumulation in cortex and subcortical white matter.4 Frank infarction with cytotoxic oedema is rarely described. However, primary endothelial dysfunction may also lead to a release of inflammatory mediators with weakening of the brain vessels’ tight junctions, followed by oedema.5 Many patients with PRES do not show typical risk factors such as hypertension, eclampsia, immunosuppression or an inflammatory state.6–10 We present the rare case of a female HIV-infected patient with a long history of antiretroviral treatment (ART), an undetectable HIV viral load and a high CD4 cell count. No classical risk factors for PRES were present. In contrast to the cases of HIV-infected patients with PRES published so far,11–15 our patient suffered neither from advanced immunodeficiency nor from opportunistic infection. However, it is conceivable that the impaired cerebrovascular reactivity, which persists even in treated and virally suppressed HIV₋infected individuals, and the persistent immune activation in these patients may represent an undetected risk factor for the development of PRES.16 17
Case presentation
A 51-year-old woman infected with HIV, who had been on first-line ART (zidovudine, lamivudine and abacavir) for 16 years, was admitted to hospital with fever, neck stiffness and altered mental status. She had a Glasgow Coma Scale of 12 and was febrile (38.4°C) on admission. Her blood pressure (114/74 mm Hg), pulse (92 beats/min) and respiratory rate (17 breaths/min) were within the normal range. Besides the HIV infection, she had a history of chronic obstructive pulmonary disease (treated with inhaled corticosteroids), an idiopathic pulmonary embolism 3 months before admission (treated with rivaroxaban) and previous history of intravenous drug abuse. For the past 16 years, the patient’s HIV status had been clinically and immunologically stable with no evidence of opportunistic diseases.
The results of the laboratory tests at the time of her admission were: CD4 count 401 cells/µL, HIV viral load below the level of detection (<20 copies/mL), as it had been in the years before. The patient had a normal leucocyte count (7300x10^9/L), slightly elevated liver enzymes (aspartate aminotransferase 152 U/L, alanine aminotransferase 99 U/L) and inflammation parameters (C reactive protein, 22 mg/L) and a creatinine level of 138 μmol/L. Blood cultures remained sterile.
Initially, we suspected meningoencephalitis and initiated empirical treatment with ceftriaxone, amoxicillin, vancomycin and acyclovir in combination with systemic corticosteroids.
The patient recovered completely within 2 days.
After stopping the oral anticoagulation, a lumbar puncture as a diagnosis of exclusion was performed 3 days after admission: no elevation of the cell count (1.0 leucocytesx10^9/L), the protein level (0.18 g/L) or the lactate level was detected. Therefore, the antimicrobial treatment was stopped.
However, 4 days after admission, the patient reported bilateral visual impairment accompanied by severe headache and subsequently suffered a tonic–clonic epileptic seizure. The ophthalmological examination revealed a bitemporal hemianopsia, visual agnosia, especially prosopagnosia, but no abnormal findings on a split lamp examination. Blood pressure was 200/120 mm Hg during this episode.
A contrast-enhanced cerebral CT scan revealed bilateral cortical and subcortical hypodense lesions in the territories of the posterior circulation (figure 1).

The axial native CT scan of the brain 4 days after hospitalisation showed relatively symmetrical bi-occipital patchy hypodense areas in the territories of the posterior circulation, cortical and subcortical, predominantly right sided.
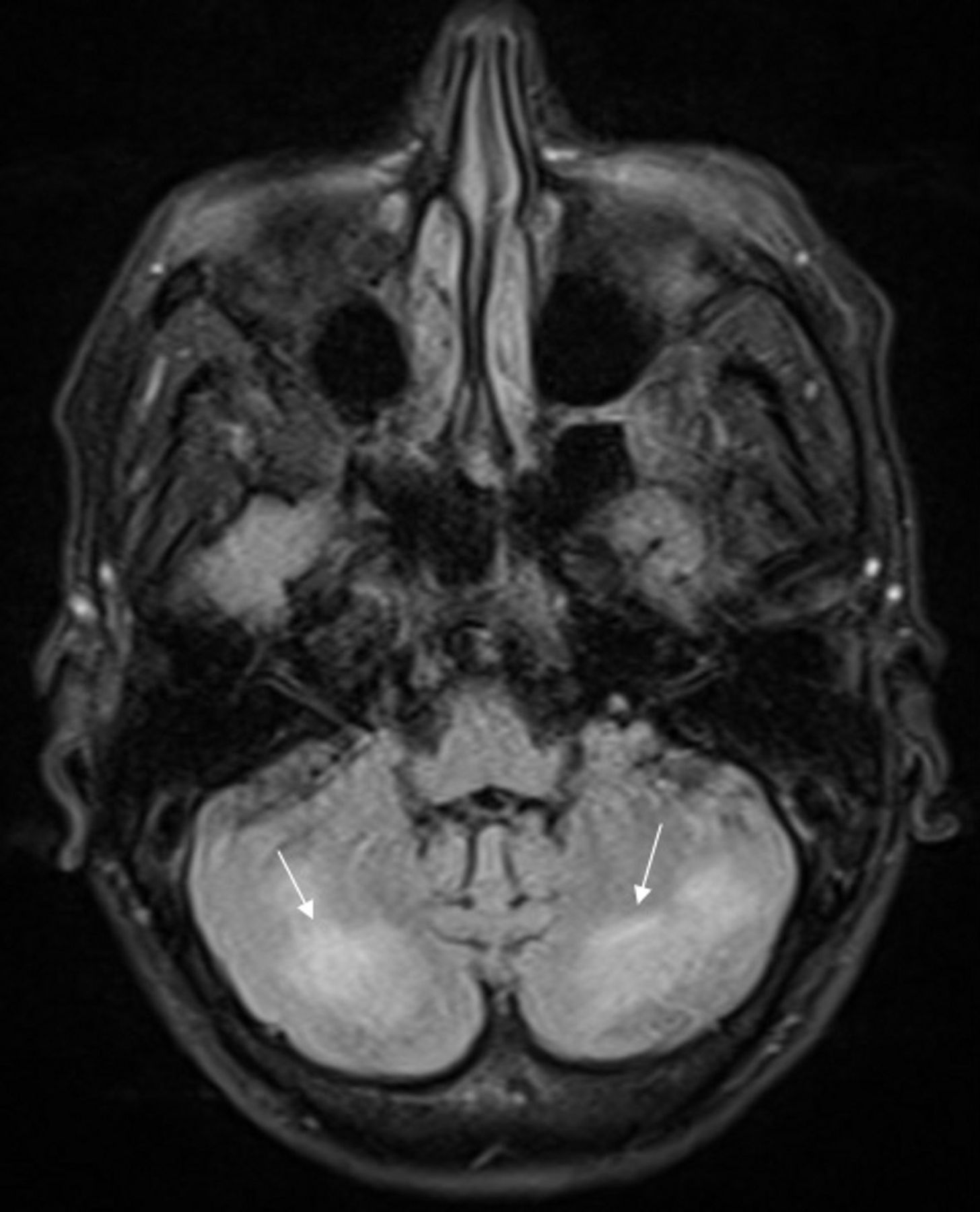
T2-weighted (T2w) and fluid-attenuated inversion recovery (FLAIR) magnetic resonance imaging (MRI) of the brain showed patchy hyperintense signal alterations—asymmetric bilateral cortical and subcortical parieto-occipital—with associated diffusion restriction (figures 2 and 3). Additionally, infratentorial large asymmetric patchy T2w and FLAIR hyperintensities were noted in both cerebellar hemispheres. The lesions showed neither contrast medium uptake nor blooming artefacts (eg, haemorrhage or calcifications).

In line with the CT scan, the MRI of the brain (axial FLAIR) revealed symmetrical, T2w and FLAIR patchy hyperintense signal alterations, asymmetric bilateral cortical and subcortical parieto-occipital. FLAIR, fluid-attenuated inversion recovery; T2w, T2 weighted.
{kind=link}
{kind=link}
{kind=link}
The MRI of the brain (axial FLAIR) demonstrated, in addition to the supratentorial hyperintense lesions, large asymmetric confluent hyperintensities in both cerebellar hemispheres. FLAIR, fluid-attenuated inversion recovery.
The electroencephalogram reinforced these findings, showing moderate decelerating foci in the left hemisphere with lateralised periodic discharges and bi-occipital spike–wave complexes with no signs of convulsive status epilepticus.
Echocardiography and ECG performed 1 month before admission had been normal and showed no signs of hypertensive cardiomyopathy.
Outcome and follow-up
After initiation of antiepileptic and antihypertensive treatment with levetiracetam and amlodipine, respectively, the patient’s neurological symptoms improved immediately. She was discharged after 8 days with no further neurological symptoms and a normal creatinine level. Antihypertensive therapy was stopped after a few days because of hypotonia. The patient remained asymptomatic and normotensive during a follow-up period of 1 year.
Discussion
PRES is characterised by headache, nausea, alteration of consciousness, seizures and visual disturbance. Brain imaging (CT and/or MRI) reveals characteristic white-matter vasogenic oedema predominantly affecting the parietal and occipital lobes.2 3
Two main hypotheses about the pathophysiology of PRES have been proposed. The more widely held theory suggests a breakdown of the autoregulatory system due to uncontrolled hypertension and subsequent hyperperfusion. The second theory is that activation of the autoregulatory system is caused by hypertension, and this results in vasoconstriction of brain vessels followed by hypoperfusion, brain ischaemia and subsequent fluid leakage.4 However, a certain proportion of patients with PRES do not have hypertension. Therefore, a third, more recent, theory about the pathophysiology of PRES, focusing on inflammatory processes, has gained attention. Activation of the immune system as well as endothelial dysfunction can lead to a release of leucocytes and tumour necrosis factor alpha. This, in turn, stimulates the expression of vascular endothelial growth factor. By this means, the tight junctions of the brain vessels are weakened and brain oedema ensues. According to this theory, hypertension seems to be an ancillary phenomenon.1 5
However, case reports and case series suggest that PRES is mostly associated with arterial hypertension, especially in the presence of (pre-)eclampsia, autoimmune disease, hypomagnesaemia, end-stage kidney disease or non-steroid immunosuppressive therapy.6–10 Classical risk factors for PRES were absent in our patient. Uncontrolled hypertension had never been documented previously or in the follow-up period and was only present during the symptomatic phase, suggesting that hypertension was an attendant phenomenon or a consequence of increased sympathetic activation, the tonic–clonic epileptic seizure and the PRES-induced brain oedema. However, as the patient was febrile at admission, we cannot exclude the possibility that an inflammatory syndrome may have played a role in the development of the PRES. Cases of PRES caused by systemic corticosteroids have also been described.18 19
Since 2002, PRES in HIV-positive patients has been described in a few case reports. Risk factors in the HIV-positive population were heterogeneous and included uncontrolled and untreated HIV infection,20 opportunistic infections in patients on tuberculosis and ART cotherapy,15 21 22arterial hypertension, end-stage renal disease,14 23 and thrombotic thrombocytopenic purpura.24 Most of the HIV-infected patients described in these case reports had advanced immunodeficiency with a CD4 count varying from 28 to 290/μL, and few of them were patients on ART with low or undetectable HIV viral load.15 The diversity of the published cases makes it impossible to determine the exact role of HIV or ART in the development of PRES and does not allow any definitive conclusion as to its pathogenesis or causality.
IRIS, an immune reconstitution inflammatory syndrome involving neurological structures, was excluded as a cause of PRES in our immunovirologically stable patient. PRES is not a manifestation of IRIS, which develops in HIV-infected patients with pre-existing infection at initiation of ART with rapid improvement of immune function. It remains unclear if long-term exposure to the combination ART with three nucleoside reverse transcriptase inhibitors exclusively, antiretroviral agents known to induce mitochondrial damage in endothelial cells, may be a cofactor contributing to endothelial dysfunction and PRES.
Although the endothelial dysfunction improves after the initiation of ART, the cerebrovascular reactivity and the systemic inflammation do not revert to normal levels even if the HIV viral loads are undetectable in patients on ART.16 17 25 It is conceivable that these factors predisposed our patient, who had no other obvious risk factors, to develop PRES.
In summary, our case highlights how the identification of classical trigger factors for the development of PRES in HIV-positive patients may be difficult. Based on pathophysiological considerations we hypothesise that HIV infection may play a role in the pathogenesis of PRES even in virologically suppressed individuals. To conclusively evaluate the role of HIV in the pathogenesis of PRES, epidemiological studies would inevitably be needed.
Learning points
Posterior reversible encephalopathy syndrome (PRES) is a rare syndrome characterised by the development of a bilateral subcortical vasogenic cerebral oedema, which mainly affects the occipital lobe.
PRES can occur in HIV-infected patients who have no other predisposing factors and in the absence of active virus replication or opportunistic infection.
Pathophysiological considerations may raise the hypothesis that HIV infection could be a previously unknown risk factor for PRES.
References
Footnotes
Contributors BB collected all the references, wrote the main part of the case report and contributed to the study design. FW contributed to the part on neuroradiology and wrote the neuroradiology subsection. CH and GW were responsible for supervision and correction and also contributed to the background knowledge of HIV in our case.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.