Article Text

Statistics from Altmetric.com
Description
Non-tuberculous mycobacteriosis most frequently presents as chronic lung disease.1 Delayed diagnosis or even misdiagnosis occurs due to a great similarity in its clinical presentation to tuberculosis.2 Treatment often seems unprofitable since it is complex and prolonged, poorly tolerated and frequently ineffective in the elimination of the disease.3
The authors present a 68-year-old woman with a history of pulmonary tuberculosis 1 year before, for which she only completed 6 weeks of treatment as well as follow-up, having abandoned both as she believed they went against her culture and religion. She was admitted with productive cough, weakness and weight loss. Blood tests revealed anaemia, thrombocytosis, elevated inflammatory markers, severe hypoalbuminaemia and negative HIV serology. The chest X-ray (figure 1) showed two cavities in the right lung and a consolidation in the left lower lobe. The chest CT scan (figures 2 and 3) showed right upper lobe pneumatocele with multiple dispersed thick-walled lung cavitations and multiple diffuse confluent nodules, diffuse reticulonodular interstitial infiltrates, multifocal bronchiectasis and several mediastinal lymph nodes, some with central necrosis. Tuberculosis reactivation was suspected. Although sputum acid-fast stain was negative, quantitative culture of bronchoalveolar lavage fluid was positive for Mycobacterium intracellulare. Treatment was started with azithromycin, rifampicin, ethambutol and amikacin, with progressive clinical improvement.

Chest X-ray. Two cavities in the right lung and a consolidation in the left lower lobe.

CT scan. Transversal plan—right upper lobe pneumatocele with multiple dispersed thick-walled lung cavitations.
{kind=link}
{kind=link}
{kind=link}
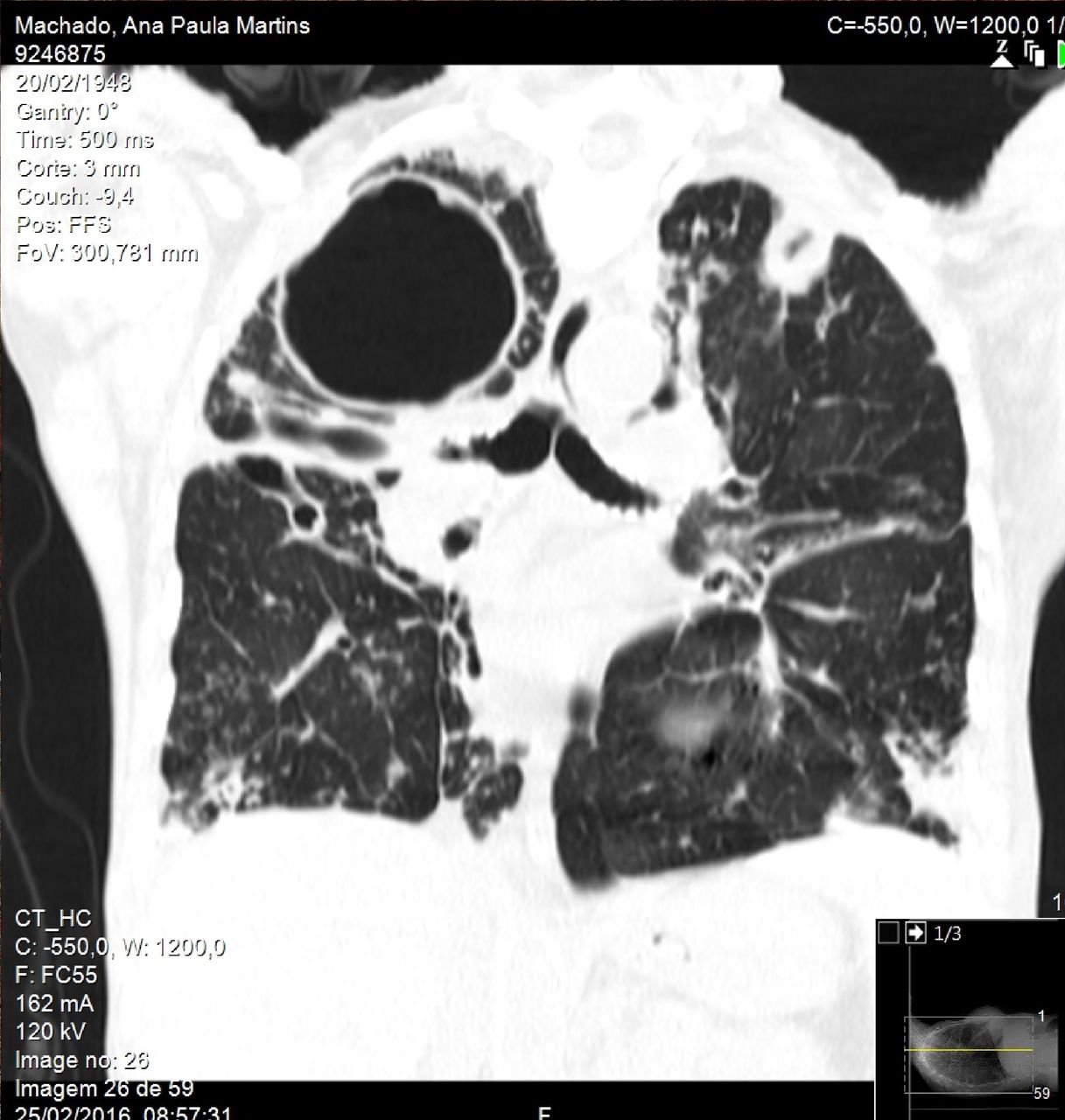
CT scan. Coronal plan—right upper lobe pneumatocele with multiple dispersed thick-walled lung cavitations and multiple diffuse confluent nodules, diffuse reticulonodular interstitial infiltrates, multifocal bronchiectasis and several mediastinal lymph nodes, some with central necrosis.
These striking images are the result of a rare infectious disease in an immunocompetent patient. Incomplete adherence to treatment has been identified as an extremely important factor in the control of mycobacterial infections as well as a major obstacle in the eradication of the disease.2
Learning points
Non-tuberculous mycobacteriosis is an infectious disease that has a complex and prolonged treatment, which contributes to poor therapeutic compliance.
Imaging is fundamental for diagnosis: the American Thoracic Society and Infectious Disease Society of America’s diagnostic criteria for non-tuberculous mycobacterial pulmonary infections include both: (1) imaging studies consistent with pulmonary disease and (2) recurrent isolation of mycobacteria from sputum or isolated from at least one bronchial wash in a symptomatic patient.
Footnotes
Contributors AIP: planning, conduct, reporting. IN: acquisition of data or analysis. GC and IMN: conception and design.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.