Article Text

Statistics from Altmetric.com
Description
A 43-year-old woman G4 P2101 at 36 weeks of gestation presented to the labour floor with non-reactive fetal heart tracing and decreased fetal movement. She had a second-trimester ultrasound showing intrauterine growth retardation (IUGR). Patient had a history of hypothyroidism, two fetal demises at term and a planned preterm delivery at 34 weeks of gestation via caesarean section. Workup was negative for thrombophilia (lupus anticoagulant, anticardiolipin, anti-b2-glycoprotein, factor V Leiden, protein S, protein C, G20210 mutation, antithrombin III, antinuclear antibodies) and infectious diseases. Placental pathology following her second fetal demise revealed chorioamnionitis and necrotising funisitis with negative amniotic fluid cultures. There was no information regarding umbilical cord (UC) length or entanglements in previous pregnancies.
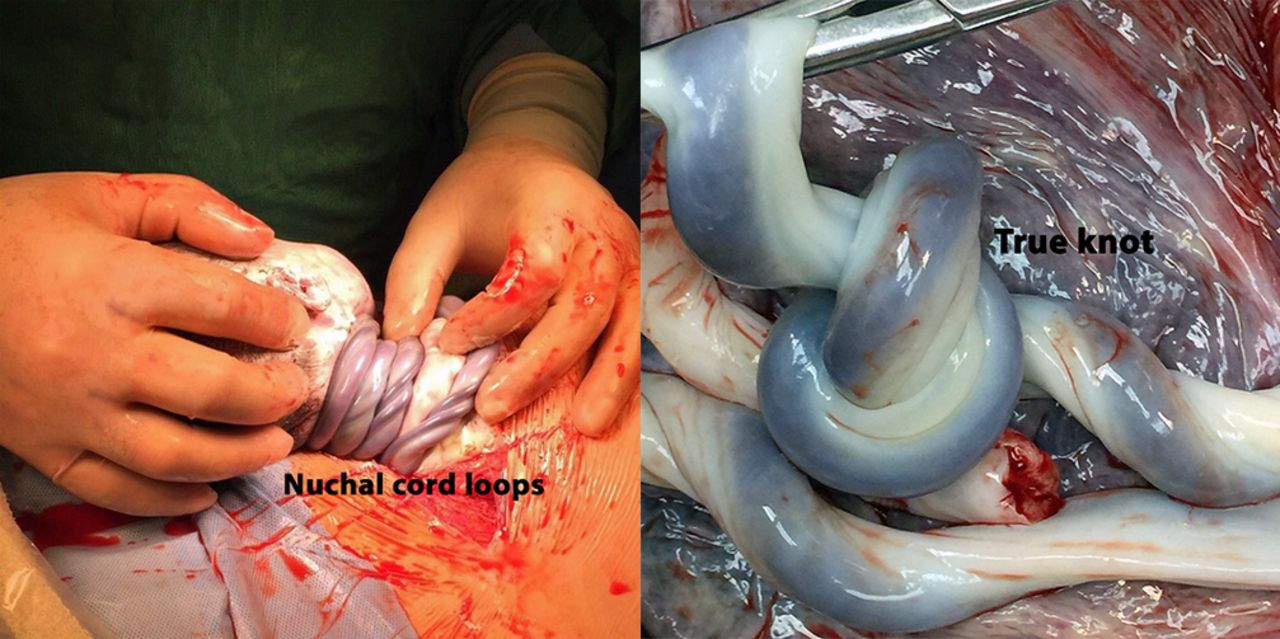
Given her history and the current non-reactive fetal heart tracing, the patient was taken for emergency caesarean delivery. A female infant was born with four loops of nuchal cord and a true knot (figure 1). Apgar scores were 7 at 1 min and 9 at 5 and 10 min. Baby weighed 1550 g. Examination of the placenta showed an excessively long umbilical cord (ELUC) measuring 93 cm. A normal UC is 55–61 cm long.

{kind=link}
Long umbilical cord with four nuchal cord loops (left) and true knot (right).
Long umbilical cords are present in 4% of placentae and pose a higher risk for cord entanglement (ie, true knots or cord loops around the neck or body parts), circulatory stasis and vascular thrombosis.1 This can cause perinatal complications, IUGR, neurological damage and fetal death. Mothers with a history of an ELUC are at increased risk of a long cord in subsequent pregnancies.1
The most common cord entanglement is nuchal cord with an incidence of 15%–34%; single loop 24%–28% and multiple loops 0.5%–3.3%.2 During the third trimester, two-dimensional sonography can detect a nuchal cord with a sensitivity of 85% and specificity of 89%.3 A single nuchal cord is not associated with any adverse perinatal outcome. However, Kong et al3 found a higher incidence of fetal distress and emergency caesarean deliveries with three loops of nuchal cords or more.
True knots are reported in 0.4%–1.2% of deliveries.2 A long UC, gestational diabetes, polyhydramnios and multiparity increase the incidence of a true knot. Although not all true knots lead to perinatal problems, they have been associated with IUGR, fetal distress, fetal hypoxia, perinatal mortality, long-term neurological damage and caesarean delivery.1 3 4 In one study, the OR for emergency caesarean deliveries due to non-reassuring fetal heart rate was 2.7 for true knot and 2.9 for multiple UC loops, respectively.4
Patient’s history of term pregnancies with fetal demise, and her negative workup, left us wondering if an ELUC associated with cord entanglements had occurred in previous pregnancies. Currently, there are no guidelines on counselling and management of patients with a true knot or nuchal cord diagnosed by antenatal sonography. Reporting these findings can lead to parental anxiety and potential medicolegal implications without improving outcomes. This case illustrates the association between an extremely long UC, cord entanglement, intrauterine growth restriction, possibility of fetal demise and need for emergency delivery.
Learning points
Excessively long umbilical cord can lead to cord entanglement.
Cord entanglement can lead to perinatal complications.
Antenatal diagnosis of multiple cord entanglements should alert the medical team to the possibility of emergency delivery.
Footnotes
Contributors RZ was involved in care of the patient, writing and editing the manuscript. FGS was invovled in writing and editing manuscript and image.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.