Article Text

Statistics from Altmetric.com
Description
This is an 81-year-old man with a history of small bowel carcinoid. He was undergoing routine surveillance (every 6 months) CT chest, abdomen and pelvis with contrast, which showed an incidental left breast mass in the lower inner quadrant, 12×9 mm concerning for breast neoplasm, there was left axillary lymphadenopathy (LAD) as well (figure 1). Correlation with clinical examination, mammography and ultrasound were recommended. A left breast ultrasound noted a hypoechoic irregular mass with indistinct margins, 7 mm in size at the 10 o’clock position on the left breast, 3 cm from the nipple (figure 2). Breast imaging-reporting and data system (BI-RADS) category 4. Bilateral mammogram demonstrated a 1.3 cm irregular shaped mass at the 10 o’clock position of the left breast. No lymphadenopathy (LAD) was noted on the mammogram or ultrasound. It was categorised as BI-RADS 5 on the mammogram. Bilateral axillary ultrasonography was obtained to evaluate for LAD and biopsy, but no evidence of malignancy was seen and no nodes were deemed necessary for biopsy. He then underwent left breast lumpectomy with histopathology. T1acN0M0, grade 1, stage IA, 1.3×1.2×1.0 cm with 0/10 mitoses/hpf. Margins were negative, closest 4–5 mm anteriorly. Microscopy showed (figures 3 and 4) a multinodular appearance, it was composed of pleomorphic polygonal cells with abundant cytoplasm and nuclear pleomorphism consisting of nuclear enlargement, nuclear multiplication and multinucleation. There was increased cellularity towards the periphery of the nodule. However, there was no significant mitotic activity or necrosis. Morphologically, it was a pleomorphic tumour with extensive hyalinising fibrosis. It was composed of polygonal and epithelial cells with abundant cytoplasm and nuclear pleomorphism including cells with large lobulated nuclei and multinucleation. It appeared to have infiltrative growth pattern at the periphery. The neoplastic cells were diffusely and strongly positive for vimentin with the positive oestrogen and progesterone receptor supporting the diagnosis of pleomorphic sarcoma (figure 5). A diagnosis of low-grade pleomorphic sarcoma (grade 1) was established after getting a second opinion. He is now planned to receive adjuvant radiation therapy. Pleomorphic sarcoma is a rare histologically heterogeneous non-epithelial neoplasm that arises from the mesenchymal tissue within the breast.1 It constitutes for less than 5% of all sarcomas in adults and rarely seen in the breast. It is uncommon in men, mainly seen in women over 64 years of age. Immunohistochemistry is vital to define histogenesis of the lesion and to differentiate undifferentiated carcinoma from mesenchymal neoplasia after the exclusion of epithelial neoplasia. The role of adjuvant treatment with chemotherapy and radiation is unclear.2 It is known to have an aggressive clinical course and high rates of recurrence and metastasis. Close follow-up is recommended.

CT of the chest showing an asymmetric left breast mass in the lower inner quadrant, 12×9 mm with left axillary lymphadenopathy.

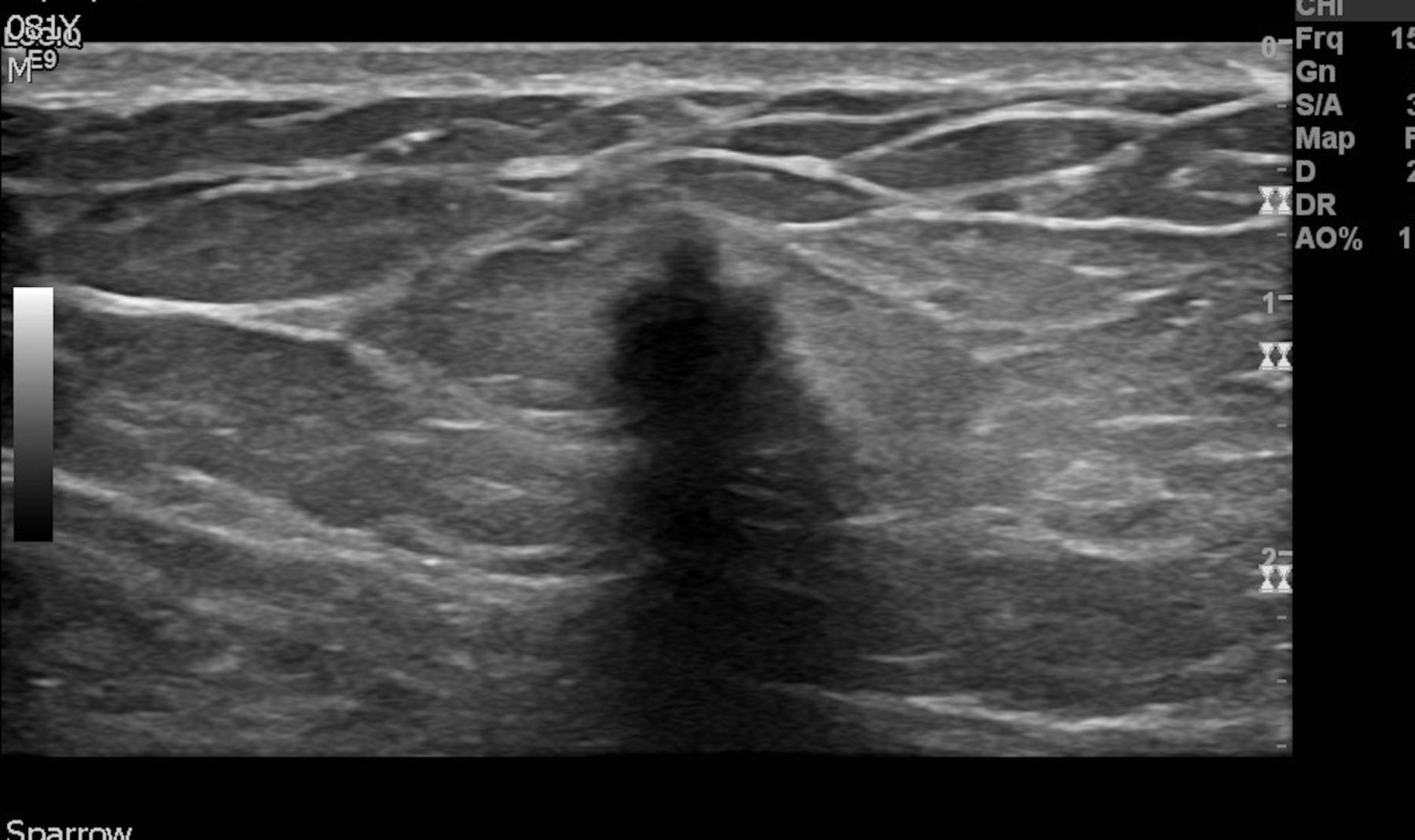
Ultrasound of the breast showing hypoechoic irregular mass with indistinct margins.

Histopathology—H&E stain 40× showing mitotic figure.

Histopathology—H&E stain 40× showing pleomorphic nuclei.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical staining positive with vimentin.
Learning points
Pleomorphic sarcoma of the breast is uncommon, and it is extremely rare in the male population.
Due to its aggressive behaviour and high rates of recurrence and metastasis, a close follow-up is recommended.
Footnotes
Contributors MPR prepared the manuscript, obtained consent. VKM assisted with literature search. SK assisted with the literature search and writing manuscript. EBM took pictures of the pathology slides and edited the pathology part of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.