Article Text

Statistics from Altmetric.com
Description
A 69-year-old woman without medical history, was admitted in our emergency department for acute respiratory distress. Two weeks prior to admission, she had undergone an endovenous foam sclerotherapy of a right saphenous branch with aetoxisclerol 2%. Afterwards, she complained of progressive dyspnoea and right thoracic pain. On arrival at the emergency department, the patient was noted to have cyanosis, a respiratory rate of 35 breaths/min and oxygen saturation of 90% despite high-flow face mask oxygen administration. Heart rate was 115 beats/min and blood pressure was 140/65 mm Hg. On physical examination, superficial thrombosis of a right saphenous branch was noted (figure 1). Laboratory studies demonstrated an elevation of markers of myocardial injuries and right ventricular dysfunction with a troponin I level of 1968 ng/L (reference value <16 ng/L) and brain natriuretic protein level of 541 ng/L (reference value <100 ng/L). Arterial blood gas showed the following: pH, 7.42; Po2, 86 mm Hg; Pco2, 37 mm Hg. ECG revealed sinus tachycardia and ST-T wave depression in inferior and lateral leads. Bedside transthoracic echocardiogram (TTE) showed an acute pulmonary heart disease with dilation of the right ventricle (RV), associated with a large floating thrombus in the right atrium (online supplementary video 1 and supplementary video 2). Initial estimated pulmonary artery systolic pressure (PASP) was evaluated at 55 mm Hg and the right ventricle/left ventricle ratio was 1.1. Left ventricular function was preserved. Immediate intravenous unfractionated heparin was done with close activated clotting time (ACT) monitoring. After pulmonary embolism specialised team concertation, thrombolysis was not considered because of preserved haemodynamic condition. On day 1, control TTE showed migration of the thrombus in the pulmonary artery. PASP was elevated and stable at 55 mm Hg. Subsequent chest CT angiography was realised and showed proximal and bilateral pulmonary embolism with dilation of the RV (figures 2 and 3). Hypoxaemia worsened during the first 24 hours after admission and was supported by high-flow face mask oxygen administration. Despite low bleeding risk, thrombolysis was not considered because haemodynamic condition remained, in contrast, stable. Initial and profound hypoxaemia was related to pulmonary embolism, infarction and pulmonary infection without microbiological documentation. Pulmonary function improved progressively and the evolution was favourable. Control TEE before discharge showed the regression of acute pulmonary heart disease signs and the PASP decreased to 37 mm Hg. The patient was discharged 3 weeks after admission with warfarin. The patient was asymptomatic and TEE remained normal at 6 months of follow-up.
Supplementary file 1
Supplementary file 2

Physical examination showed superficial thrombosis of a right saphenous branch.

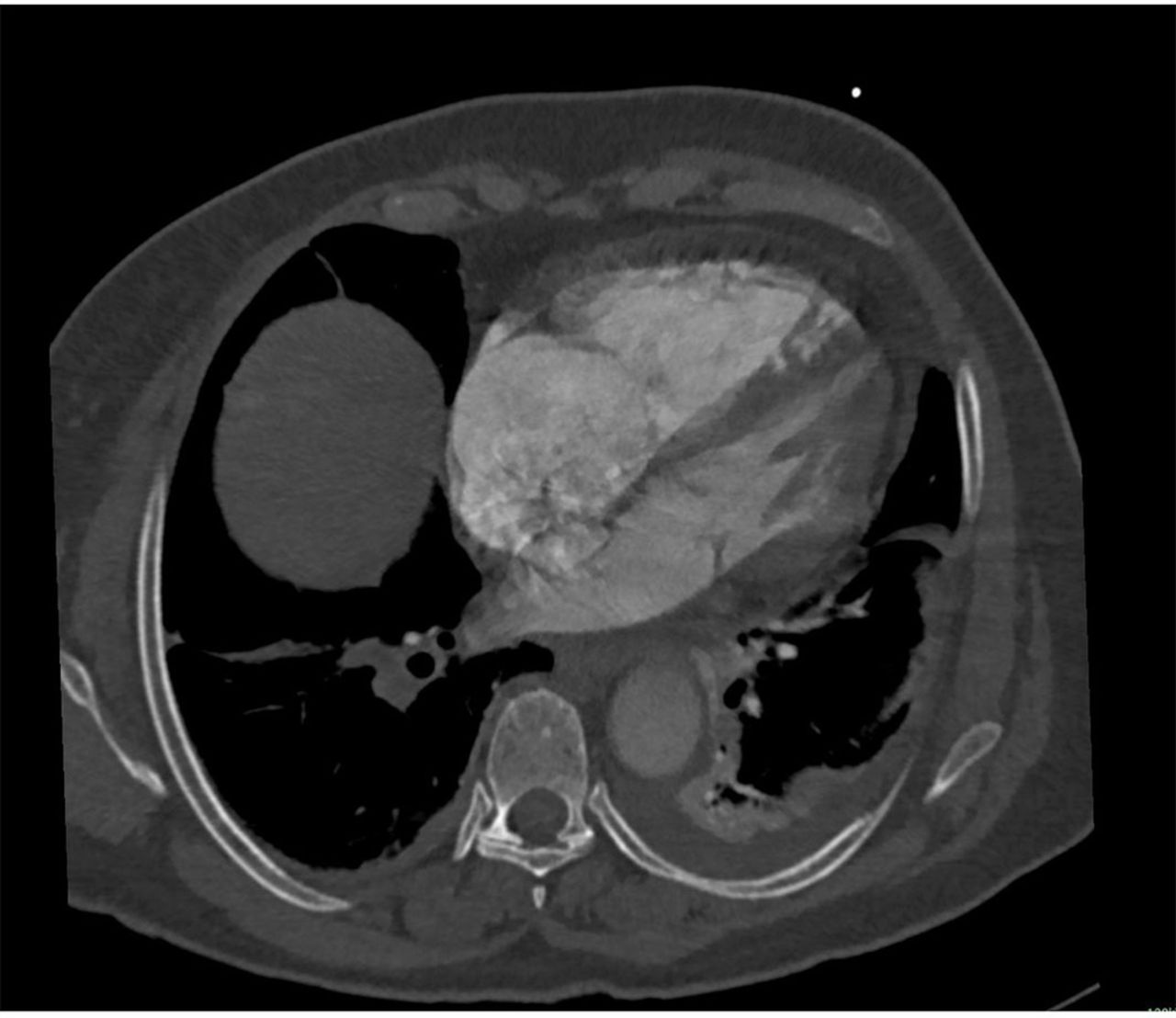
Proximal and bilateral pulmonary embolism on chest CT angiography.

{kind=link}
{kind=link}
{kind=link}
Dilation of the right ventricle on chest CT angiography.
The rate of venous thrombosis following endovenous foam sclerotherapy is low. Deep venous thrombosis rate is reported to be less than 1%, and PE rate is 0.1%.1 2 Prevention of such complications is achieved by wearing compression stockings all day during 3 weeks after the procedure. Independently of the aetiology, patients with PE associated with RV dysfunction and myocardial injury (intermediate-risk to high-risk pulmonary embolism), thrombolytic therapy should be considered if clinical signs of haemodynamic decompensation appeared.3–5 Among patients who appear haemodynamically stable, the presence of a right heart thrombi is associated with high early mortality, evaluating between 20% and 30% in patients treated by heparin independently of further thrombolysis administration.6 7 Because of low incidence and conflicting results, there are no clear recommendations for the management of this subset of patients.5 Surgical embolectomy, interventional approach, thrombolysis therapy or heparin alone can be considered. Treatment decision is highly related to local expertise and heart team discussion, as reflected by our case.
Learning points
Right heart thrombus is a rare condition.
The mortality rate is high, even with preserved haemodynamic condition.
There are no data regarding the best medical therapy (heparin alone vs thrombolytic therapy).
There is no comparison between medical and invasive strategy (intervention or surgery).
Footnotes
Contributors DL, SH, RD and VS contributed to the planning, conducting and reporting of the work described in this article. VS is responsible for the overall content.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.