Article Text

Statistics from Altmetric.com
Description
A 25-year-old man with HIV infection was admitted with generalised abdominal pain, fever and vomits. He had been diagnosed a few months earlier with disseminated Mycobacterium avium Complex (MAC) infection through a bone marrow biopsy but had abandoned all treatments. Blood tests showed pancytopenia with CD4 lymphocyte count of 0,034x109/L (normal 0.41–1,59 x109/L) and a raised alkaline phosphatase of 541 IU/L (normal 40–150 IU/L) with otherwise normal liver tests. Abdominal ultrasound and CT showed multiple coeliac and lateroaortic lymphadenopathies as well as a homogeneous hepatosplenomegaly; the oesophagogastroduodenoscopy (OGD) showed only a congestive bulbar mucosa. The patient was then referred for a capsule endoscopy: the small bowel mucosa was oedematous, with prominent lymphangiectasia and multiple ulcers, more exuberant proximally, that were suggestive of MAC infection (figure 1) (see video 1 in the online supplementary file 1). Distal duodenal biopsies showed a macrophage infiltration in the lamina propria (figure 2), but acid-fast bacilli were not evident with Ziehl-Neelsen staining. Whipple’s disease was excluded through a negative PCR for Tropheryma whippelii. Macrophage infiltration is considered a typical feature of disseminated MAC infection; so in this patient with a previously confirmed MAC diagnosis and with symptoms and endoscopic aspects suggestive of the disease, we assumed that the manifestations were due to disseminated MAC. The patient had already been restarted on antiretroviral therapy and symptoms resolved completely after institution of triple anti-MAC therapy with clarithromycin, ethambutol and rifabutin that was continued for 12 months.
Supplementary file 1
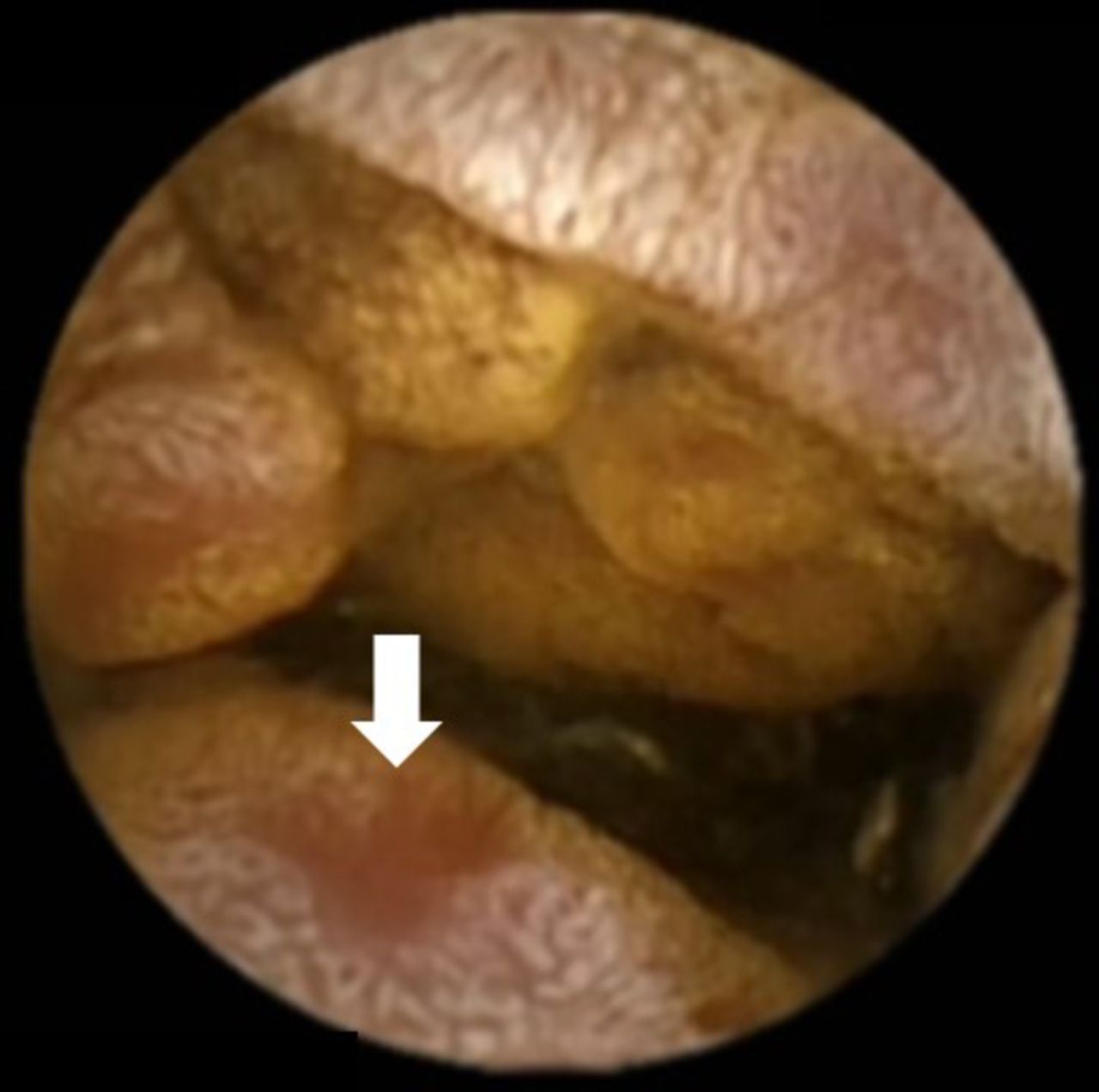
Proximal small bowel with mucosal oedema, lymphangiectasia and ulcer (white arrow).

{kind=link}
{kind=link}
Duodenal biopsies showing macrophage infiltration in the lamina propria (H&E).
Disseminated MAC infection is an AIDS-defining opportunistic infection. It usually occurs when CD4 lymphocyte counts are below 50 cells/µL. MAC is a ubiquitous organism in the environment that can enter the body through inhalation or ingestion. It can penetrate the gastrointestinal (GI) mucosa where it is phagocytosed by macrophages; however, these cells cannot destroy the organism and it eventually spreads via lymphatics and blood stream.1 GI involvement in disseminated disease occurs more often in the duodenum, although it can involve any section of the gut. Endoscopic features associated with GI involvement in disseminated MAC infection include mucosal oedema, friability, whitish nodules, erosions/ulcerations and lymphangiectasia.2 GI biopsies in patients with AIDS usually show multiple macrophages filled with acid-fast bacilli.1 Treatment must include a combination of 2–3 antibiotics effective against MAC.3
With the introduction of effective antiretroviral therapy, the incidence of disseminated MAC infection has diminished among people with AIDS. However, it is still possible to find some cases in our daily practice, especially in patients with poor adherence to therapy. For this reason, it is essential to be familiarised with the endoscopic aspects of the infection. In this case report, the aspects on OGD were not considered relevant; only after capsule endoscopy did we saw some aspects that suggested the disease and prompted the performance of duodenal biopsies, since the most exuberant findings were located past the duodenum. These biopsies, although non-diagnostic, were compatible with MAC infection and, together with the clinical history, allowed the exclusion of other entities. So, although not always required for the diagnosis, capsule endoscopy might enable a timely diagnosis in some cases, preventing the morbidity and mortality associated with this condition.
Learning points
Disseminated Mycobacterium avium complex infection is an AIDS-defining opportunistic infection that can involve the gastrointestinal tract.
Suggestive endoscopic aspects include mucosal oedema, friability, whitish nodules, erosions/ulcerations and lymphangiectasia.
Capsule endoscopy may suggest the diagnosis in patients with normal oesophagogastroduodenoscopy.
Footnotes
Contributors AMV wrote the paper; FV made the endoscopic diagnosis; AJC made the histological diagnosis and HG reviewed the paper and provided references.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.