Article Text

Statistics from Altmetric.com
Description
A 32-year-old man presented with a 3-day history of abdominal pain, vomiting and diarrhoea. He was afebrile and haemodynamically stable (saturating at 97% on air with a respiratory rate of 15, his blood pressure was 117/65 with a heart rate of 78 bpm). Clinical examination revealed right iliac fossa tenderness with localised guarding. His inflammatory markers were raised (white cell count 21 x109/L , neutrophils 16 and C-reactive protein 26). He was diagnosed with acute appendicitis and had an emergency open appendectomy. The operative findings were a periappendicular mass with a necrotic tip of appendix and pus within the abdomen.
Unfortunately he had a complex postoperative course. He developed paralytic ileus by day 3 and was managed conservatively via insertion of a nasogastric tube, rehydration with intravenous fluid and correction of his electrolyte imbalance. By day 6 he became febrile (39°), increasingly short of breath with a grossly distended non-tender abdomen, warranting an urgent CT abdomen and pelvis. Imaging identified dilated loops of small bowel with extensive intramural air, large amount of air in the intrahepatic and portal venous system and small pockets of air within the superior mesenteric vein. The ascending colon was dilated but the remaining large bowel loops appeared normal. Trace fluid was present in the pelvis. This impressive rare picture is of pneumatosis intestinalis (PI) with extensive hepatic portal venous gas (HPVG) (figures 1 and 2).
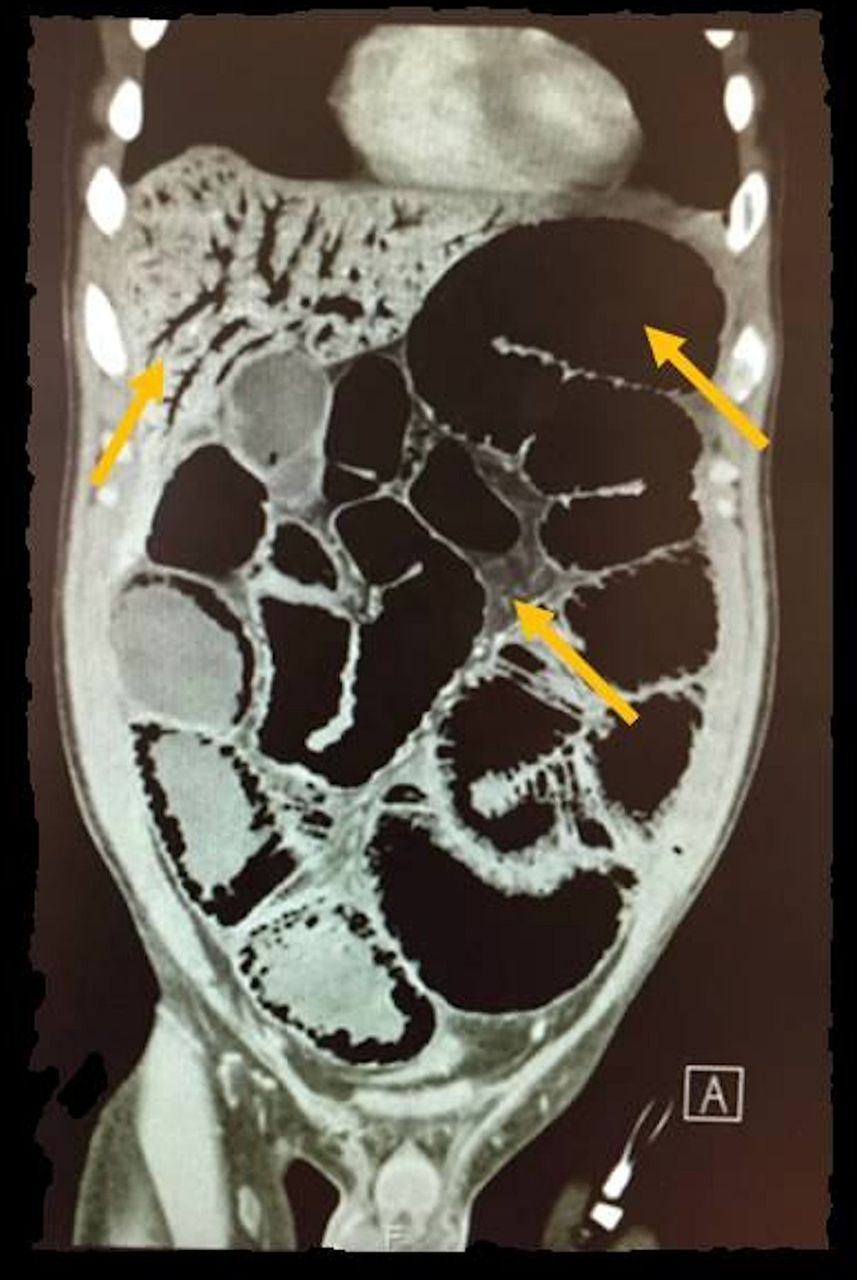
CT scan (coronal view): extensive intrahepatic air, air also within bowel wall with dilated bowel loops (arrows).

CT scan (axial view): enhanced bowel wall with intramural air (arrows).
The PI was initially medically managed with hyperbaric oxygen, antibiotics and an elemental diet; unfortunately with little clinical improvement. Two days later, the abdomen, now painful, continued to distend. His arterial blood gas showed a lactate of 17. A repeat CT scan now revealed a pneumoperitoneum, ascites and peritonitis (figure 3). An emergency laparotomy revealed a 2 mm mid-jejunum perforation which was closed with primary sutures with washout of the peritoneal cavity. Following a prolonged hospital stay, requiring Intensive treatment unit (ITU) support, he eventually recovered and was discharged 36 days later. He was reviewed in the outpatient clinic 3 months later and reported remaining well after discharge and is continuing to be rehabilitated.

{kind=link}
{kind=link}
{kind=link}
CT scan (axial view): ascites with multiple air bubbles, a complication of pneumatosis intestinalis (arrows).
PI is a rare radiological finding resulting from gas cysts accumulating within the bowel wall.1 An array of aetiologies exist including underlying disease, medication and trauma.2 Hence the management of this phenomenon greatly varies from a cautious conservative approach to surgical intervention guided by frequent review of the patient’s clinical condition as demonstrated via our case; a dilemma for the surgeon.
HPVG is another rare sign resulting from accumulation of air within the hepatic portal system with most cases being related to mesenteric ischaemia.3 CT imaging, therefore, is an extremely valuable tool in identifying this pathology, and in cases of suspected bowel ischaemia or infarction an urgent explorative laparotomy is mandatory. Clinicians should be aware of these uncommon signs and the challenges they may pose.
Learning points
Pneumatosis intestinalis is not a clinical diagnosis but a radiological finding and its underlying cause should be explored and treated accordingly.
A number of complications are associated with pneumatosis intestinalis including pneumoperitoneum, ascites and peritonitis and require urgent surgical intervention.
Cases of pneumatosis intestinalis associated with portomesenteric venous gas are indicative of ischaemia and can lead to bowel perforation.
Footnotes
Contributors FA researched the topic and wrote the case. AA and SZ both helped with the research and proofreading of the case report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.