Article Text

Statistics from Altmetric.com
Description
A 5-month-old female infant presented with an 8 days duration of fever and irritability. In the previous 48 hours, she developed a rash around her umbilicus with reduced feeding and wet nappies (figure 1). She was born at 38+3/40 weeks gestation by caesarean section for breech presentation. At 4 months of age, she had gastro-oesophageal reflux. She initially presented to the general practitioner (GP) at 3 months of age with redness around the umbilicus and dried clots in the centre without any swelling. She had no fever and was otherwise well. Initial treatment given by GP included a 1-week course of oral flucloxacillin for provisional diagnosis of infected umbilical granuloma. This seemed to have resolved her symptoms.

Clinical photograph showing a diffuse periumbilical erythema.
The baby was referred for paediatric assessment by her GP with recurrent symptoms mentioned above. On examination, periumbilical erythema was present with no obvious tenderness. A diffuse superficial swelling with induration was noted to the left side of the umbilicus. This had enlarged over a few hours rapidly, measuring 3×3 cm from twice its original size.
Blood results showed a raised C-reactive protein of 72 mg/dL and platelets 719 x 109/L. White cell count of 32.3 x 109/L and neutrophils 15.9×1000/mm3 were also raised consistent with infection.
She was started on intravenous flucloxacillin. A clinical diagnosis of urachal sinus leading to infection of the urachal cyst or embryonic remnants of vitellointestinal tract was considered and an ultrasound requested. Ultrasound showed a sinus tract leading to an infected cyst (figure 2). The CT abdomen was performed to delineate the anatomy further and it confirmed the presence of an urachal sinus leading to an infected and complex urachal cyst measuring 5.6×2.8×4.2 cm (figure 3). Intravenous flucloxacillin resolved the umbilical redness and the underlying infection.
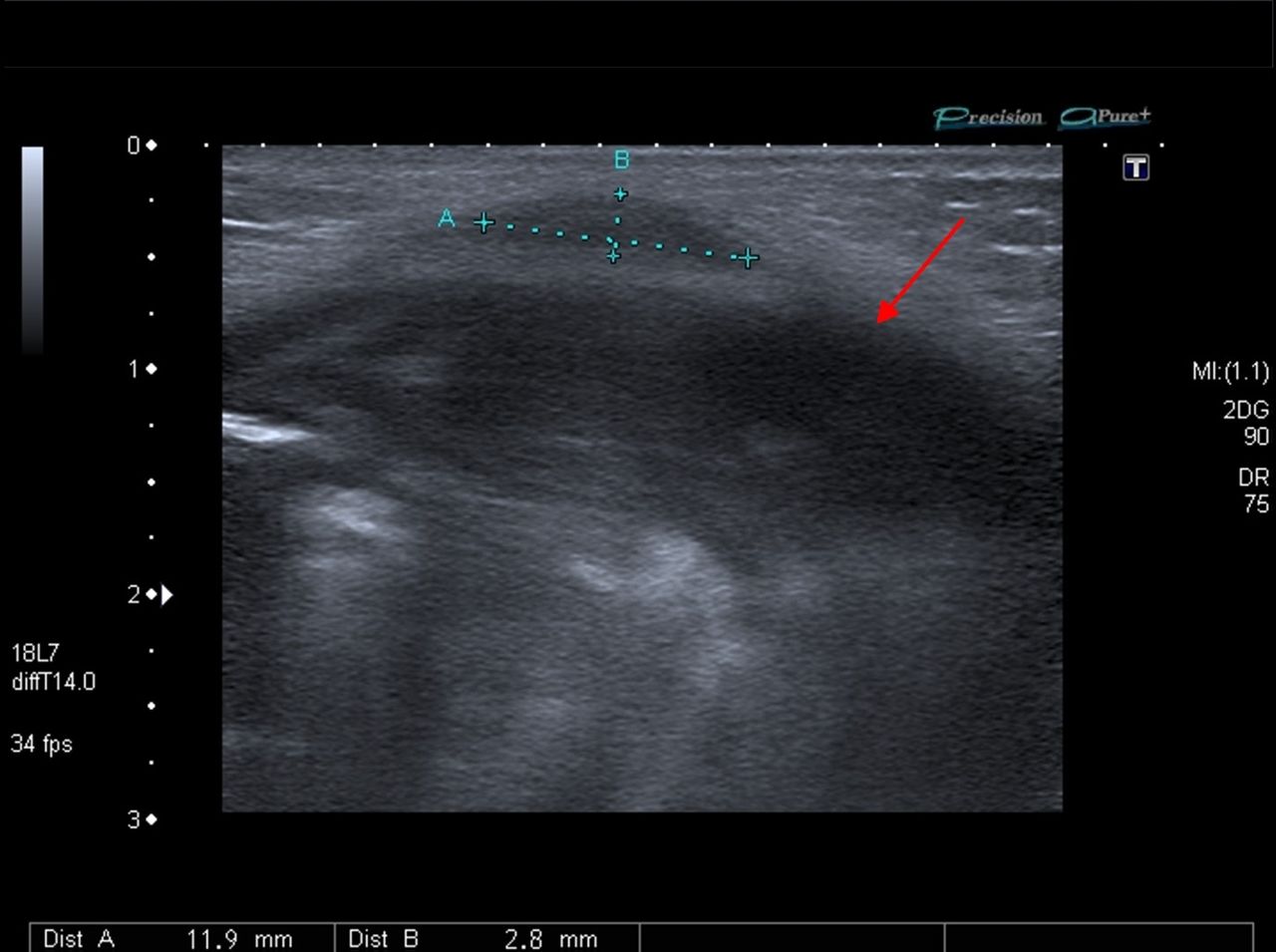
Ultrasound abdomen of the periumbilical region. The red arrow showing a complex mass just to the left of the midline.

{kind=link}
{kind=link}
{kind=link}
Abdominal CT showing a multicystic mass extending from urinary bladder inferiorly to the level of the umbilicus (red arrow).
No visible swelling or abscess was observed after 4 days. She was discharged home with paediatric urology follow-up for possible further surgery and excision of the cyst.
Urachal sinus and cysts are rare. They arise from incomplete regression of the fetal urachus between the umbilicus and bladder. They are usually silent clinically until infection, calculi or cysts develop.1 In rare occasions, they can present late into adulthood as an infection.2 3 Rare cases of adenocarcinoma have been described. Due to their non-specific presentation, diagnosis can be missed if not actively considered.4 A similar case with prolapsed urachal sinus leading to the pyourachus has been reported recently.5
Learning points
Urachal sinus and cysts are rare and can present as recurring periumbilical sepsis.
A non-resolving umbilical granuloma or rapidly expanding umbilical or periumbilical mass should alert the clinician to possibility of this condition.
If missed for a number of years, a potential for malignant change exists.
Footnotes
Contributors KWT was involved in the case, reviewed the case notes and wrote the article. LN helped to identify and annotate the radiological images. HB was the overseeing consultant.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.