Article Text

Statistics from Altmetric.com
Description
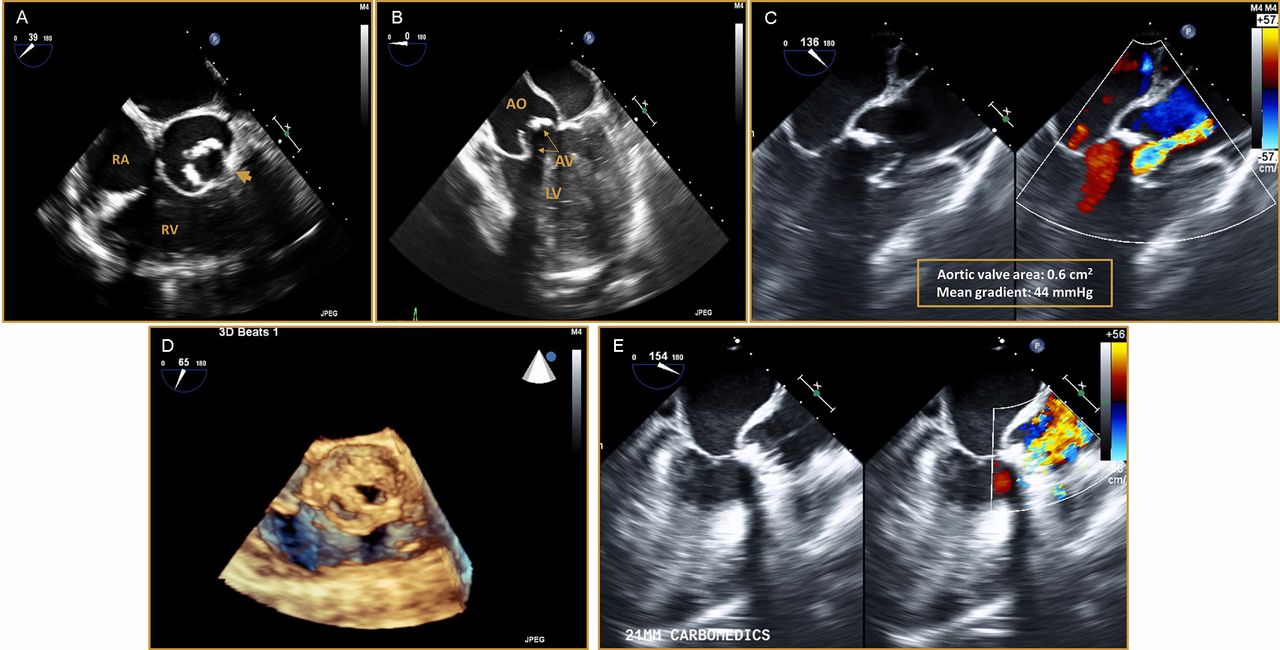
A 24-year-old man with a known history of horseshoe kidney leading to end-stage renal disease, scoliosis and small ventricular septal defect consistent with VACTERL association, who presented with worsening dyspnoea on exertion. Transthoracic echocardiogram (TTE) showed a unicuspid aortic valve (UAV) with severe aortic stenosis (AS) (valve area of 0.6 cm2 and mean gradient of 44 mm Hg). TTE also showed moderate aortic insufficiency and severely reduced left ventricular systolic function with estimated ejection fraction of 20%. Transoesophageal echocardiography (TEE) confirmed a UAV with single commissure located anteriorly (figure 1A–D; online supplementary video 1 and supplementary video 2) and severe AS (figure 1B, C). In preparation for surgical repair, chest CT angiogram showed dilated ascending aorta measuring 4 cm with no evidence of aortic dissection. The patient underwent aortic valve replacement surgery with 21 mm CarboMedics mechanical valve. TEE showed a well-seated prosthesis without evidence of paravalvular leak (figure 1E). The patient had an uneventful recovery and was discharged after close monitoring for 1 week.

{kind=link}
Two-dimensional transoesophageal echocardiography (TEE) images.(A) Short-axis view reveals a unicuspid aortic valve with a single commissure located anteriorly (arrow). (B) Long-axis view shows stenotic aortic valve (AV) and mildly dilated ascending aorta (AO). (C) Long-axis view with Doppler color indicating severe aortic valve stenosis. (D) Three-dimensional TEE image displays a unicommissural unicuspid aortic valve with a poor excursion of the cusp during systole. (E) Two-dimensional long-axis view TEE image showing prosthetic aortic valve with normal Doppler.
UAV is a rare form of congenital heart disease seen in approximately 0.02% of patients referred for echocardiographic studies.1 It is susceptible to early degeneration thus resulting in aortic stenosis with or without regurgitation. Two forms of UAV have been described, the unicommissural variant which is characterised by the presence of a lateral attachment to the aorta with an eccentric orifice and the acommissural form in case of the absence of such attachment and presence of a central orifice.1 UAV has been reported to be associated with other cardiac anomalies such as aortic coarctation, ventricular septal defect, patent ductus arteriosus and aortic aneurysm.2 VACTERL association is a group of birth defects that affect multiple organ systems and typically defined by the presence of at least three of the following congenital anomalies: vertebral defects, anal atresia, cardiovascular defects, tracheo-oesophageal fistula, renal anomalies or limb abnormalities.3 To our knowledge, there is no previous report of unicuspid aortic valve as a part cardiac anomalies in VACTERL association.
Learning points
Unicuspid aortic valve is a rare congenital heart defect.
Patients with unicuspid aortic valve presented at early age with aortic valve stenosis or regurgitation.
Presence of unicuspid aortic valve in young patients should raise concerns for other congenital abnormalities.
Footnotes
Contributors MS and HMP contributed substantially to data interpretation, writing and reviewing the manuscript for important intellectual content. CA is the co-senior authors of this manuscript and had access to all the data, contributed to writing and reviewing the manuscript for important intellectual content.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.