Article Text

Statistics from Altmetric.com
- cancer intervention
- haematology (drugs and medicines)
- haematology (incl blood transfusion)
- malignant and benign haematology
Description
A 49-year-old woman with no significant medical history presented to her primary care provider for an evaluation of a new lump in her groin. She was found to have enlarged inguinal lymph nodes on the right side, and underwent extensive work-up, including testing for HIV, hepatitides, Epstein-Barr virus, cytomegalovirus and chest imaging. They were all unremarkable. Given persistence of the lymphadenopathy, the patient underwent a fine needle aspiration of one of the lymph nodes with pathology revealing a diagnosis of low-grade follicular lymphoma. Given the natural history of this slow-growing tumour, she was maintained on an observational protocol but unfortunately lost to follow-up.
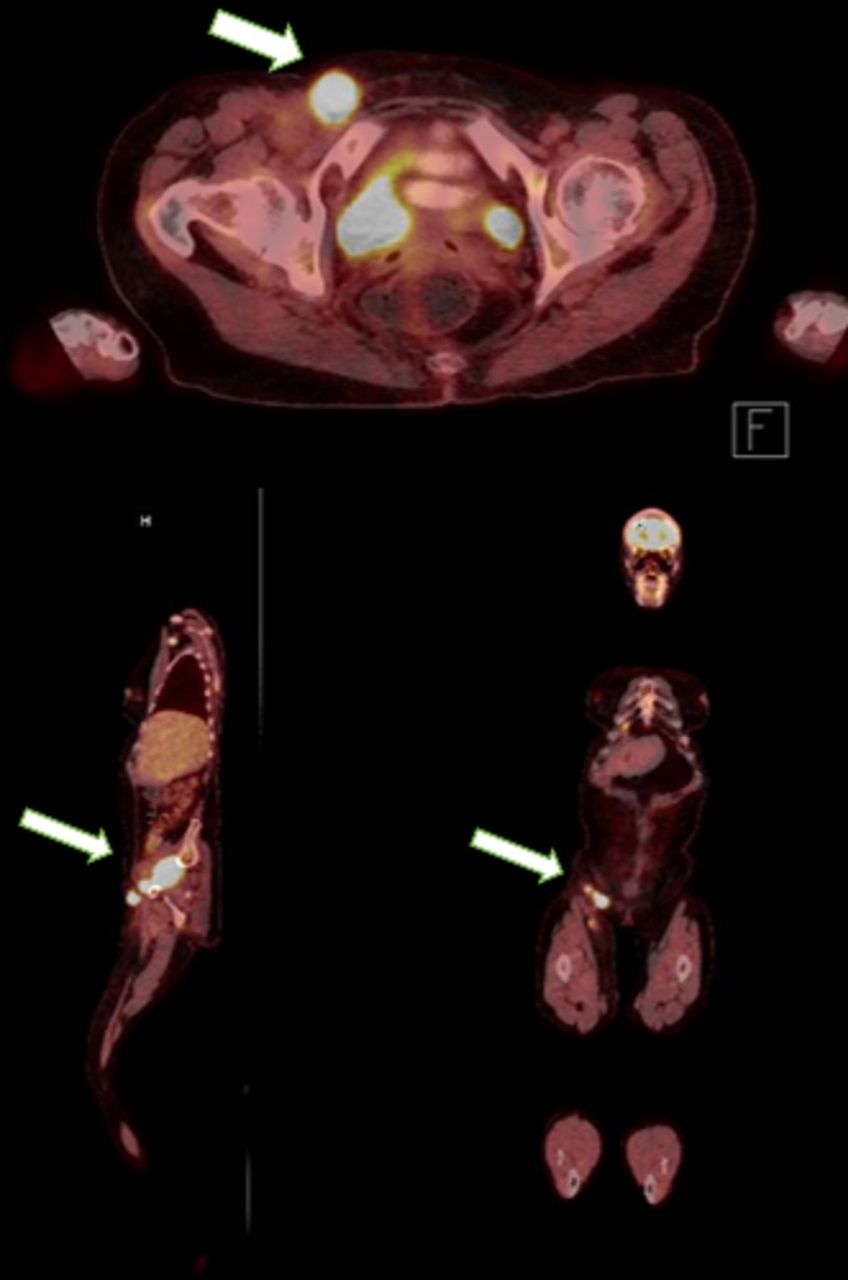
Three years later, the patient presented to the emergency department for complaints of generalised malaise as well as an enlarging right groin mass. Physical examination revealed a fungating mass with purulent drainage and an impressively pungent smell in the right inguinal area (figure 1). CT of the abdomen and pelvis with contrast revealed necrotic pockets in the mass (figure 2). A subsequent positron emission tomography (PET) scan confirmed metabolic activity in the necrotic mass (figure 3). A repeat biopsy revealed the diagnosis of diffuse large B cell lymphoma (DLBCL), germinal centre subtype. Additionally, blood cultures obtained during admission subsequently grew Escherichia coli. She was treated with piperacillin–tazobactam and narrowed to ceftriaxone when susceptibilities returned. Following clearance of her E. coli bacteraemia, chemotherapy with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone, (R-CHOP) and focused radiation to her groin were initiated.

Photograph of the patient’s right groin mass on initial presentation.
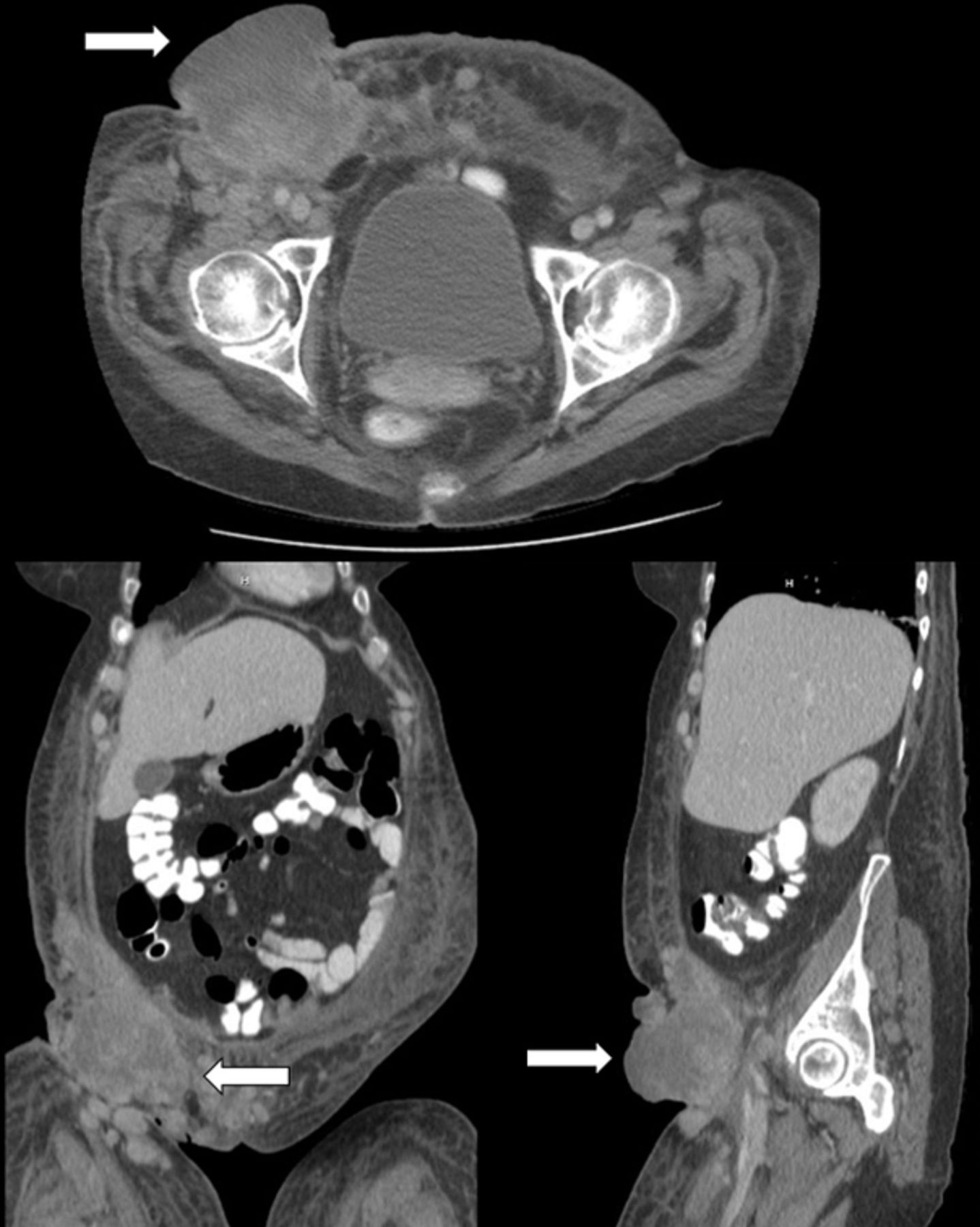
Axial, coronal and sagittal CT images of the mass (arrows depicting mass) showing enlarged nodes with necrotic pockets.

{kind=link}
{kind=link}
{kind=link}
Axial, coronal and sagittal positron emission tomography images of the mass showing increased uptake by the enlarged inguinal nodes.
Follicular lymphoma is the most common indolent non-Hodgkin’s lymphoma,1 comprising 20% to 30% of all newly diagnosed non-Hodgkin’s lymphomas in the Western world (Europe and North America). The incidence of this cancer increases with age, with the median age of diagnosis around 60.2 The treatment is dependent on staging, and asymptomatic patients with low tumour burden can often be managed with ‘watchful waiting,’ which has a freedom from treatment failure similar to patients managed upfront with rituximab-based regimens.3 There is a 3% risk of transformation to DLBCL, a more aggressive subtype of non-Hodgkin’s lymphoma, in the first 15 years after diagnosis,1 after which the risk begins to fall. While certain genetic mutations may increase the risk of transformation, no clinical features have reliably been shown to be associated with an increased risk of transformation to DLBCL.1
Bacteraemia is a significant complication in haematological malignancy, in both neutropenic and non-neutropenic patients. In one retrospective review of infectious complications in patients with aggressive mature B and T cell lymphomas, gram-negative rods represented 57% of all infectious complications; gram-positive cocci were almost always associated with indwelling lines present for the purpose of chemotherapy.4 In another retrospective study of patients with DLBCL, there was an 11% early death rate (death before 5-year follow-up), 3.6% of which was attributable to infection.5
In this article, we presented a case of a patient who initially presented with low-grade follicular lymphoma that subsequently transformed to a fungating DLBCL complicated by development of E. coli bacteraemia.
Learning points
Low-grade follicular lymphoma can often times be managed with watchful waiting.
The risk of transformation of follicular lymphoma to diffuse large B cell lymphoma, with associated formation of more aggressive nodal masses, is highest in the first 15 years after diagnosis.
In patients with aggressive lymphomas, gram-negative bacteraemia is a common complication and (even if non-neutropenic) can cause significant morbidity and mortality.
Footnotes
Contributors TC was directly involved in patient care, helped mentor the corresponding author (KB) and helped revise the case report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.