Article Text

Summary
Cold agglutinins are autoantibodies that agglutinate red blood cells at low temperatures, leading to haemagglutination and haemolysis. They are generally of no clinical significance. However, when people with cold agglutinins undergo cardiac operation with hypothermia and cold cardioplegia, they can experience complications. Thus, different perioperative management is required for such patients. We describe a 74-year-old man with cold agglutinins incidentally detected on the preoperative screening test. He had never experienced any complications or developed a haematological disease. Since cold agglutinins were incidentally detected on the preoperative test, a special strategy was used to manage the temperature of cardiopulmonary bypass (CPB) and cardioplegia. He successfully underwent normothermic cardiac operation with warm cardioplegia. A continuous retrograde hyperkalaemic infusion and intermittent antegrade infusion of warm cardioplegia with normothermic CPB is one of the best methods to avoid hypothermia and excessive activity and metabolism of the heart, and to provide a suitable operative field.
- anaesthesia
- cardiovascular medicine
- surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Cold agglutinins are autoantibodies that agglutinate red blood cells at low temperatures, leading to haemagglutination and haemolysis.1–11 They are generally of no clinical significance.1–3 5 6 8 10 11 However, when people who have cold agglutinins in their blood undergo cardiac operation under hypothermia and cold cardioplegia, they can experience complications.1 2 4 6 7 10 11 The reported incidence of cold agglutinins among screened cardiac surgical patients is low but not too rare (approximately 0.8%–4%4 6 7), and different perioperative management is required for such patients. We describe a patient with incidentally detected cold agglutinins who successfully underwent normothermic cardiac operation with warm cardioplegia.
Case presentation
A 74-year-old man was scheduled for cardiac operation because of severe mitral regurgitation and coronary stenosis. During preoperative screening, all initial preoperative routine test results were normal, except for the presence of the non-specific cold antibodies confirmed by the saline method. The direct antiglobulin test was negative for anti-immunoglobulin G, but we did not perform further testing of anti-C3. These findings had not been assessed until the preoperative evaluation by anaesthesiologists. On the basis of these indications, we postponed the operation and performed further tests, which resulted in the detection of cold agglutinins by the haemagglutination assay. The titre of the cold agglutinin was 1:512 at 4°C, and the thermal amplitude, defined as the highest temperature at which haemagglutination occurs, was 32°C. The patient had no history of anaemia, prior blood transfusion or any disease other than prostate cancer, for which he had undergone operation without complications.
Haematologists diagnosed him as having idiopathic cold agglutinin disease because of a lack of prior infection or haematological malignancy. There is no consensus on the clinical significance of the cold antibody titre and thermal amplitude that warrant appropriate precautions.1 However, he had no clinical symptoms, and his agglutinin titre was not extremely high compared with those of previously reported cases2 3; there was no indication for preoperative plasmapheresis or the administration of immunoglobulin,4 corticosteroids and alkylating agents3 and rituximab therapy.5 However, thermal amplitude, which is more important than the titre in predicting the likelihood of complications,1 6 was 32°C; therefore, management using hypothermic cardiopulmonary bypass (CPB) with cold cardioplegia would have caused the temperatures of his core, peripheral and coronary arteries to reach unsafe levels.
Therefore, we performed normothermic cardiac operation with warm cardioplegia. We usually use a single infusion of cold blood cardioplegia in an antegrade and retrograde delivery system every 30 min, which was modified from the one-dose method.12
To avoid inadequate protection of the heart due to warm conditions and excessive cardiac activity and oxygen consumption, we added a continuous retrograde hyperkalaemic infusion to the intermittent antegrade infusion of cardioplegia. The patient was protected from exposure to hypothermia using warming blankets and a fluid warming system.
Retrograde cardioplegia (36°C) was performed continuously, except when antegrade cardioplegia was administered. We used blood cardioplegia made of the patient’s blood and potassium chloride (KCl, 8–20 mEq/L). We maintained cardiac arrest during almost the entire CPB period while keeping the patient’s temperature >35°C.
The patient had uneventful intraoperative and postoperative courses, with no clinically significant haemagglutination or haemolysis.
Written informed consent was obtained from the patient for publication of this case report.
Treatment
We changed the routine CPB plan (hypothermic CPB with cold cardioplegia) to normothermic CPB with warm cardioplegia. We administered a continuous retrograde hyperkalaemic infusion and intermittent antegrade infusion of warm cardioplegia with normothermic CPB, and we tried to keep the patient warm throughout the perioperative period.
Outcome and follow-up
The operation was successfully completed without complications, and the patient has been well without any symptoms 1 year postoperatively.
Discussion
The optimal guidelines of patients with cold agglutinins undergoing CPB operation remain controversial because of the limited number of case reports. Some physicians believe that patients with low titres and low thermal amplitude antibodies may undergo CPB operation without any change in the routine management plan.1 2
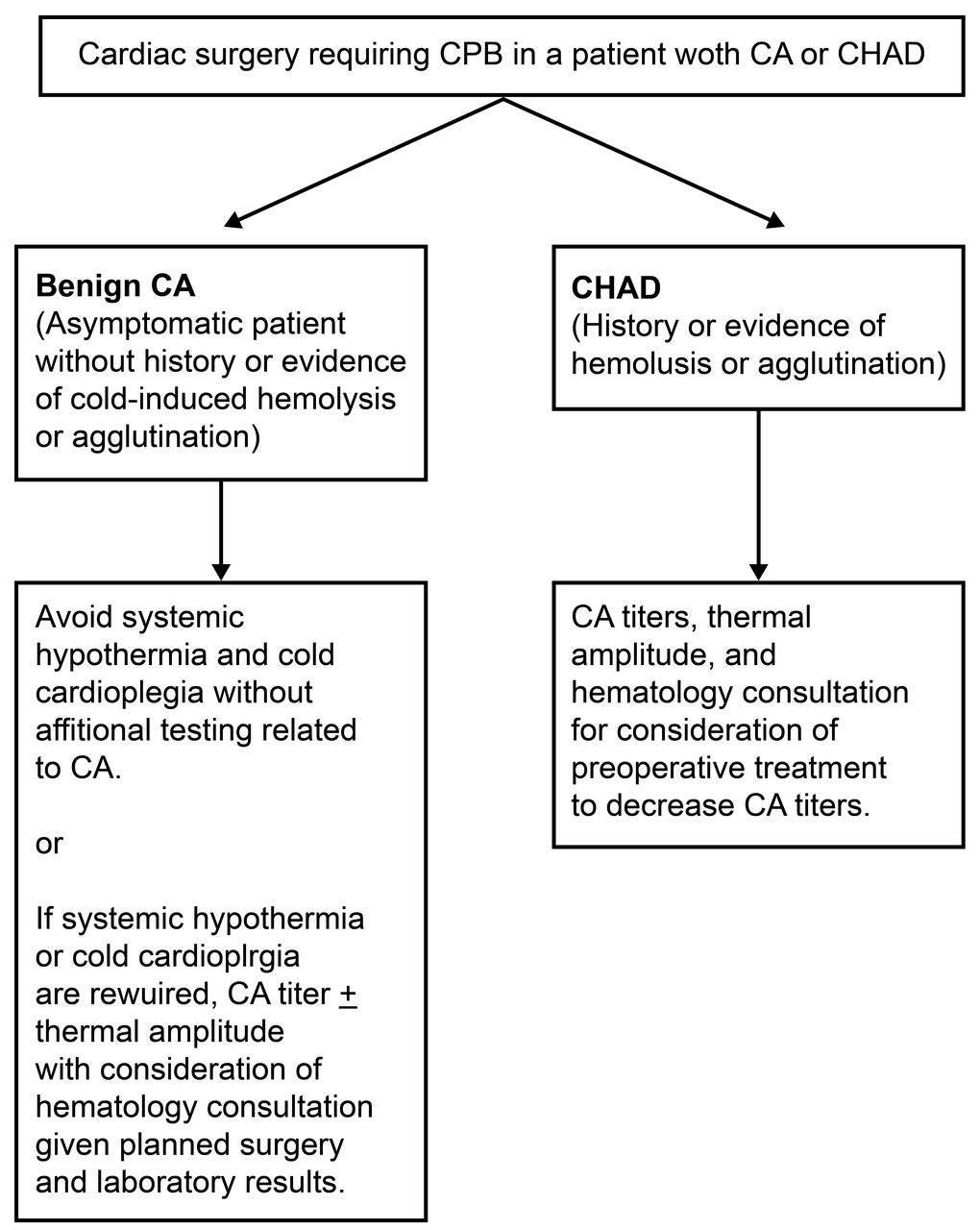
Recently, a new algorithm1 was proposed to guide preoperative testing in patients with cold agglutinins (figure 1). The authors claimed that patients with non-symptomatic cold agglutinins can safely undergo normothermic cardiac operation with warm cardioplegia at 37°C, and they may not require additional testing. The determination of titres, thermal amplitude and haematology consultation are recommended in patients when systemic hypothermia or cold cardioplegia is required in benign cold agglutinins.

Recommendations for preoperative testing and haematology consultation in patients with benign cold agglutinins and cold haemagglutinin disease. Reproduced from Barbara et al.1 CA, cold agglutinins; CHAD, cold haemagglutinin disease; CPB, cardiopulmonary bypass.
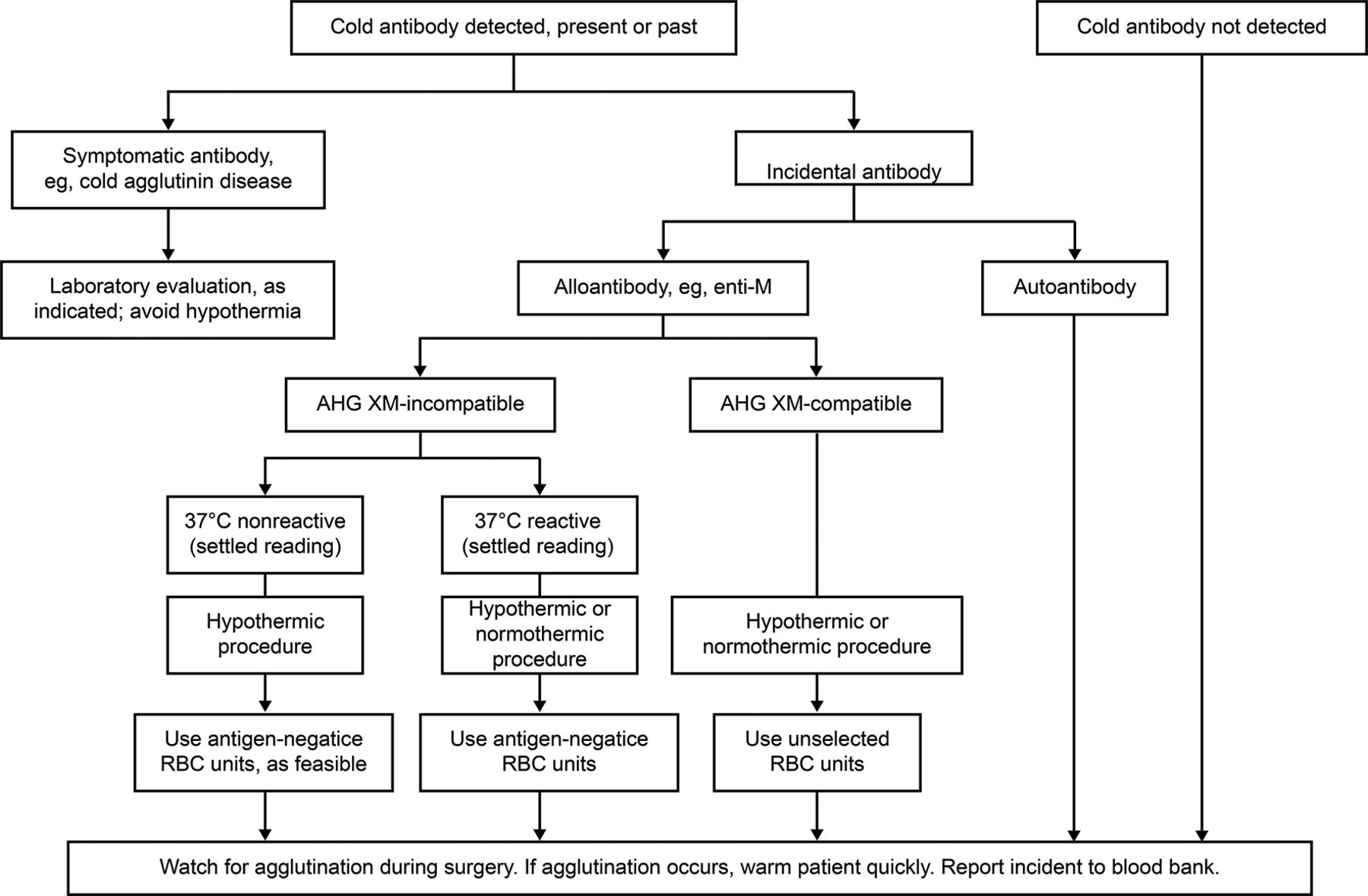
Furthermore, other authors developed guidelines2 (figure 2) for pretransfusion testing and perioperative management of patients with cold agglutinins. They claimed that if cold agglutinins are incidentally detected and are not symptomatic, standard pretransfusion testing should be performed to determine whether antigen-negative red blood cells should be used. Considering the rarity of haemagglutination among patients with cold agglutinins, they concluded that special preoperative testing protocols are neither necessary nor justified in the absence of pathogenic cold agglutinins or symptoms. Physicians now tend to exclude unnecessary examinations related to cold agglutinins preoperatively given their cost–benefit relationships.
{kind=link}
{kind=link}
Guidelines for managing patients with cold antibodies who undergo cardiovascular operation. During the preoperative visit, the patient must be evaluated for a history suggestive of pathogenic cold antibodies. Reproduced from Sapatnekar and Figueroa.2 AHG XM, antihuman globulin crossmatch; RBC, red blood cell.
Regarding temperature management, protection of the myocardium and other organs may be jeopardised under normothermic surgical conditions and warm cardioplegia. It is difficult to accurately assess adverse effects of temperature management during CPB on myocardial oxygen consumption and energy metabolism at the cellular levels. Physicians have tried to determine the best CPB temperature management, and contraindicated outcomes between normothermic and hypothermic CPB operations have been reported.13–15 According to the Clinical Practice Guidelines for Temperature Management during CPB,16 surgical teams should limit the CPB temperature to <37°C to avoid cerebral hyperthermia (class I, level C), and temperature gradients between the arterial outlet and venous inflow should not exceed <10°C to avoid generation of gaseous emboli (class I, level C). No unified agreements have been reached on this difficult topic in the normal population. The presence of cold agglutinins presents more complicated problems in optimal temperature management during CPB. According to the experts’ opinion,1 normothermic CPB operation with warm cardioplegia can be safely performed without any complications in patients with cold agglutinins. However, this disease has a special pathophysiology that is often ignored. Haemagglutination observed in patients with pathogenic cold agglutinins is not reliably correlated with the antibody titre.5 8 This phenomenon may occur in patients with titres as low as 1:32. Haemagglutination and the subsequent haemolysis caused by activated cold agglutinins have been observed in patients with low titres.9 10 This may be more hazardous during CPB under low-temperature conditions and, indeed, some lethal, irremediable cases have been reported.10 11
On the basis of past reports, we presume that patients with cold agglutinins may exhibit haemagglutination and a haemolytic crisis, even with low antibody titres and examination results that are not particularly abnormal. Complete preoperative screening for the cold antibody and direct communication with haematology specialists are required before additional tests are necessary and to avoid unexpected complications, especially if the patient is scheduled to undergo cardiac operation with CPB and could be exposed to cold conditions. Patients with a history or symptoms/signs suggesting cold agglutinin disease or the presence of any abnormal cold antibody should be referred to a haematology specialist, who would then determine the appropriate test, especially if the patient is scheduled to undergo cardiac operation with CPB and can be exposed to cold conditions.
If physicians do not know the patient’s background characteristics and do not have much experience with this disease, as in the present case, they should take the most cautious measures, for example, preoperative testing of antibody titres and thermal amplitudes, after consulting with other medical professionals. A continuous retrograde hyperkalaemic infusion and intermittent antegrade infusion of warm cardioplegia with normothermic CPB is one of the best measures for patients with unknown background characteristics and for physicians without much experience in treating this condition.
We consider that this technique can be applied as a general replacement for cold cardioplegia without risk of agglutinations and other complications, if the systemic potassium concentration and myocardial energy metabolism are controlled. Unfortunately, we could not perform comparative experiments or draw any definitive conclusions; however, we believe further case reports and discussions can lead to better management of this disease.
Patient’s perspective
I considered that by avoiding cold conditions, I would be well without complications, such as haemagglutinations and a haemolytic crisis.
Learning points
Cold agglutinins of low antibody titres can cause haemagglutination and a haemolytic crisis even in asymptomatic patients with an increased risk in cardiopulmonary bypass (CPB) operation.
Complete preoperative screening for the cold antibody and direct communication with haematology specialists are required before additional tests are necessary and to avoid unexpected complications, especially if the patient is scheduled to undergo cardiac operation with CPB and could be exposed to cold conditions.
Patients with a history or symptoms/signs suggesting cold agglutinin disease or the presence of any abnormal cold antibody should be referred to a haematology specialist, who would then determine the appropriate test, especially if the patient is scheduled to undergo cardiac operation with CPB and can be exposed to cold conditions.
Continuous retrograde infusion of hyperkalaemic warm cardioplegia with normothermic CPB in patients with cold agglutinins is one of the best methods to avoid hypothermia and excessive activity and metabolism of the heart, and to provide a suitable operative field.
This aforementioned method can be used by simply adding it to the intermittent routine administration of cardioplegia, and it is useful for physicians without much experience with this disease.
Acknowledgments
I would like to thank my colleagues, operating room staffs, and clinical engineers for their generous support, which enabled me to write this paper.
References
Footnotes
Contributors TO is the sole author of this paper and wrote the whole manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.