Article Text

Statistics from Altmetric.com
Description
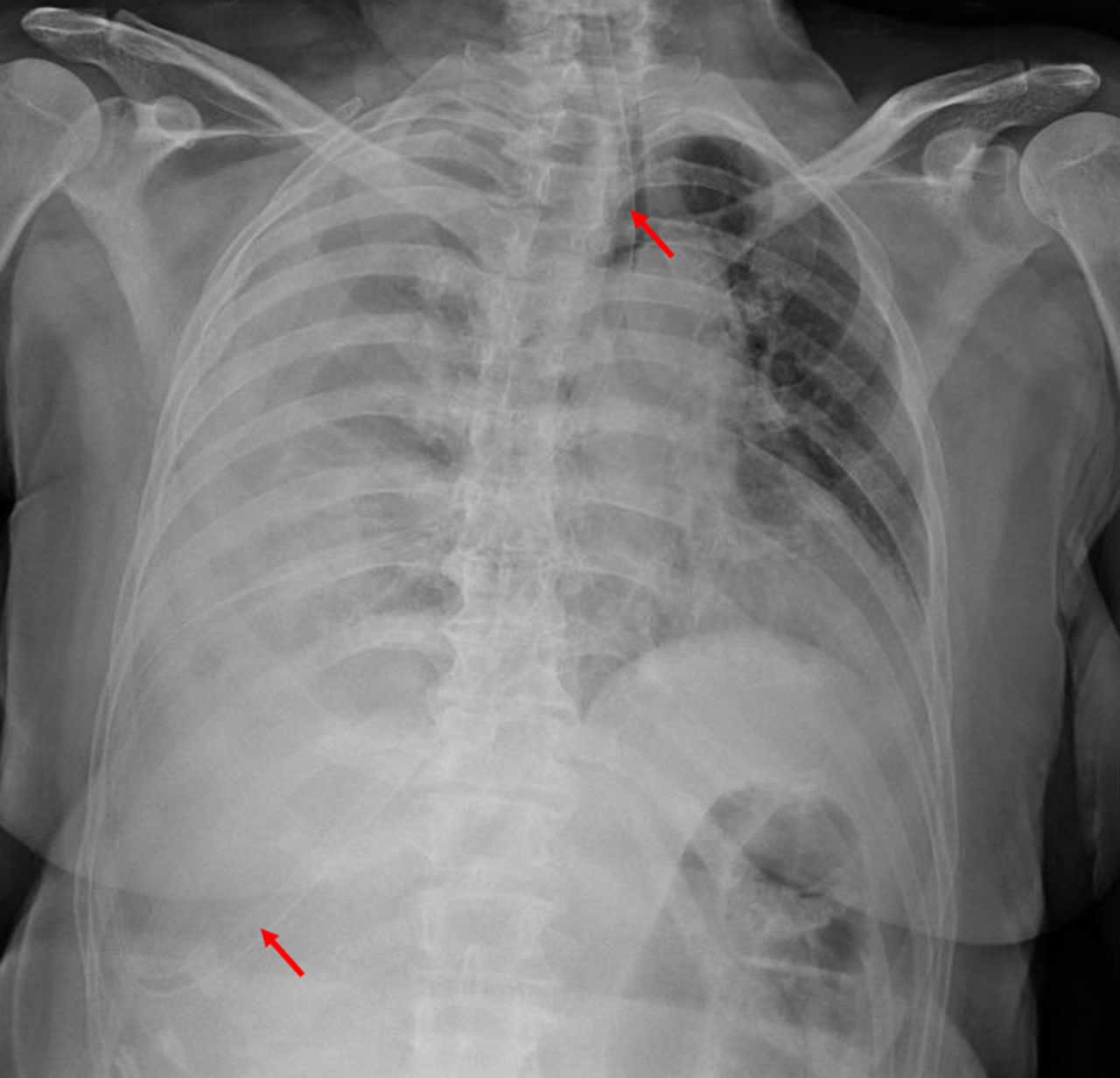
A 62-year-old woman with history of frontotemporal dementia was admitted to a Psychiatry ward due to severe insomnia. In the morning, after the admission a nasogastric tube was placed to initiate enteral feeding and medication since she was refusing all oral intake. Later that night, she was found unresponsive, dyspnoeic and with severe hypotension. Physical examination identified clinical signs of respiratory distress and decreased vesicular breath sounds on the right hemithorax. The gasometric evaluation revealed the presence of hypoxaemia and lactic acidosis. A posteroanterior chest radiograph showed a right pleural effusion and a misplaced nasogastric tube (figure 1). A thoracic CT scan revealed the presence of a right hydropneumothorax and also identified a tube inside the trachea and the right main bronchus, which perforated the lung parenchyma and ended in the pleural cavity (figure 2).

Posteroanterior chest radiograph showing right pleural effusion and a misplaced nasogastric tube (arrows).

{kind=link}
{kind=link}
Thoracic CT scan showing right hydropneumothorax and also a tube inside the trachea and the right main bronchus, which perforated the lung parenchyma and ended in the pleural cavity (arrows).
It was assumed an iatrogenic complication after nasogastric intubation. The content obtained after pleural effusion drainage was consistent with food delivered through the nasogastric tube during breakfast and lunch. The patient was submitted to a right segmental lobectomy, with no immediate complications. She has been evaluated for the last 2 years, showing no respiratory symptoms or pulmonary dysfunction. She maintains regular Psychiatry consultations due to her frontotemporal dementia.
Nasogastric intubation is associated with iatrogenic complications in up to 8% of the cases.1 The most common ones are related to the respiratory system.2 In order to prevent such accidents, the use of auxiliary techniques such as the capnography and endoscopy during nasogastric intubation is recommended.3
Learning points
Iatrogenic complications still play an important role in the daily activity in any medical institution and every clinician must be aware of them
Nasogastric intubation is not an innocuous procedure and is associated mainly with respiratory system complications
Auxiliary techniques should be used in order to prevent these kinds of complications
Footnotes
Contributors HJC was responsible for the data collection and analysis, drafting the article and final approval of the version to be published. JC was responsible for the data collection and analysis, and final approval of the version to be published. BN and MP were responsible for the critical revision and final approval of the version to be published. All authors read and approved the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.