Article Text

Statistics from Altmetric.com
Description
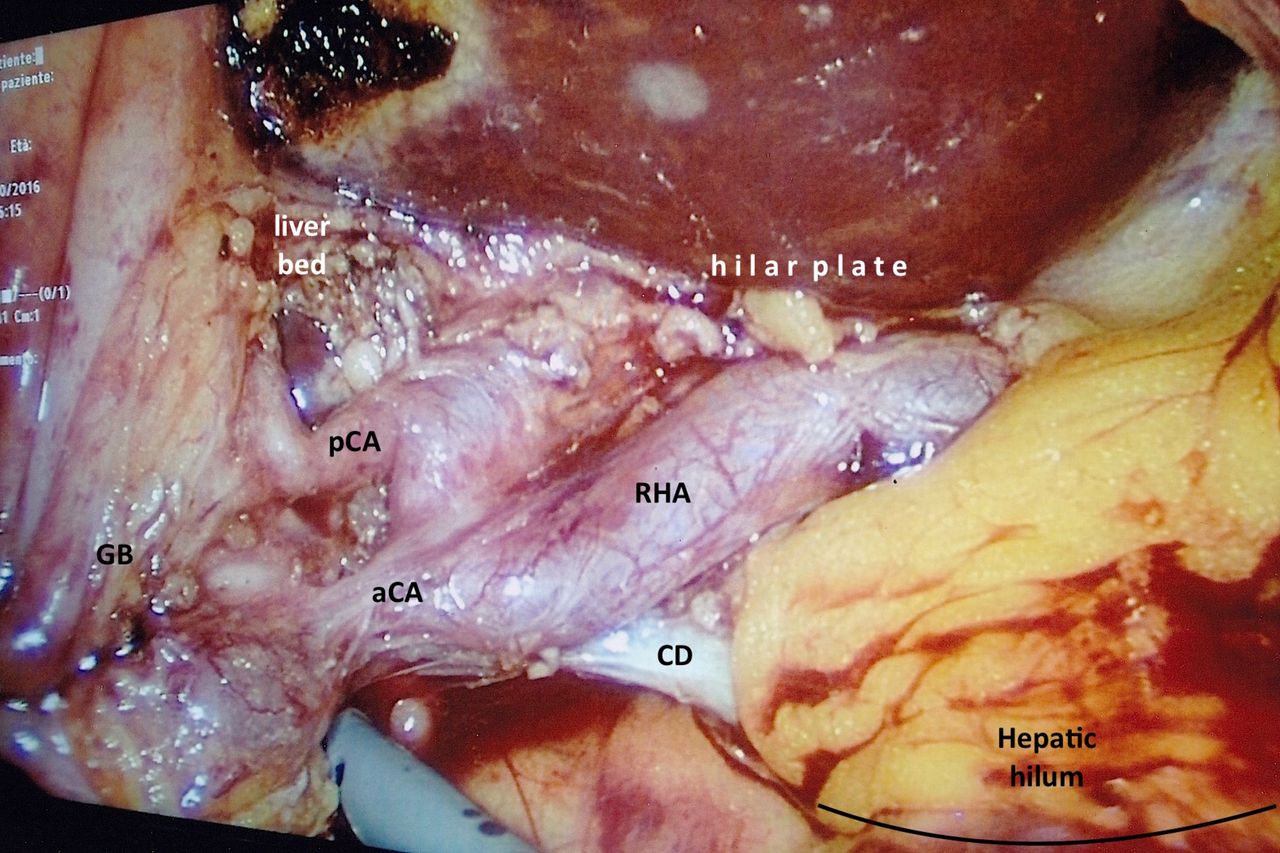
A 60-year-old woman with unremarkable medical history, underwent elective laparoscopic cholecystectomy for symptomatic cholelithiasis. A four-port technique was performed. Initial exploration of Calot’s triangle was carried out by upward traction of the fundus and lateral retraction of the Hartmann’s pouch; after dissection of the peritoneum medially at the level of the infundibulum, two tubular structures entering the gallbladder were visible, as usually expected. However, to obtain a ‘critical view of safety’,1 dissection was continued by opening up the lateral aspect of the peritoneum; hepatobiliary triangle was dissected free of areolar tissue and the bottom of the gallbladder was dissected off the lower part of the liver bed. At this stage, an anatomical variation became evident (figure 1): the right hepatic artery made a ‘caterpillar-like’ loop inside Calot’s triangle and two short cystic arteries reached the gallbladder. According to a recent review, among clinically important variations, short (<1 cm) cystic arteries are found in 9.5% and multiple cystic arteries in 8.9% of operative or anatomical cases.2 Tortuous right hepatic artery (‘caterpillar hump’) is an infrequent but potentially dangerous variation, especially when combined with short cystic arteries or variant vascular anatomy, for its position deep in the Calot’s triangle and possible termination in the cystic plate.3 In the case presented, a careful dissection aiming to the ‘critical view of safety’ and ligation close to the gallbladder avoided inadvertent division of the right hepatic artery and bleeding (figure 2). Retrograde cholecystectomy was then completed safely and postoperative course was uneventful.

Intraoperative view of right hepatic artery caterpillar hump: notice the dual short cystic arteries and how the RHA loop terminates at the hilar plate in close proximity to the liver bed. The hepatic hilum is covered by omentum. aCA, anterior cystic artery; CD, cystic duct; GB, gallbladder; pCA, posterior cystic artery; RHA, right hepatic artery.

{kind=link}
{kind=link}
Schematic view of figure 1. Relevant structures of the hepatic hilum and Calot's triangle are depicted; site of surgical dissection and division is shown (interrupted line arrow). aCA, anterior cystic artery; CD, cystic duct; CBD, common biliary duct; CHD, common hepatic duct; GB, gallbladder; pCA, posterior cystic artery; RHA, right hepatic artery.
Learning points
When performing a laparoscopic cholecystectomy, surgeons should bear in mind that anatomical variations are common in the general population.
Critical view of safety should be pursued to avoid misidentification of cystic artery or biliary ducts thus preventing iatrogenic injuries.
Acknowledgments
The authors wish to thank F. Bottazzini for the photo shooting, V. Fornoni for the drawing and Prof. G. Rossi for the support
Footnotes
Contributors AZ and GF performed the operation described in the article, AZ conceived the manuscript, GF reviewed the manuscript and edited the images.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.