Article Text

Summary
Liver trauma is a recognised rare complication of cardiopulmonary resuscitation (CPR) and may be difficult to detect. We report a case of intraperitoneal haemorrhage due to liver injury following CPR in a 50-year-old man admitted to the intensive care unit. The haemorrhage was diagnosed with focused assessment with sonography for trauma (FAST). FAST can rapidly and easily diagnose liver injury. FAST is recommended for excluding haemoperitoneum in patients who are haemodynamically unstable after resuscitation.
- trauma
- liver disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Liver trauma is a rare complication of cardiopulmonary resuscitation (CPR) that can be difficult to detect.1 We report a case of intraperitoneal haemorrhage due to liver injury following CPR. On arrival to the intensive care unit (ICU), the patient was diagnosed with liver damage via focused assessment with sonography for trauma (FAST). The present case illustrates the utility of FAST for excluding haemoperitoneum in patients who are hemodynamically unstable after resuscitation.
Case presentation
A 50-year-old man suffered a seizure, which was witnessed by bystanders, while walking on the street. The patient became unresponsive and the bystanders performed CPR at the scene. Emergency services arrived 10 min later; however, automated external defibrillator did not work. The emergency personnel commenced CPR and the patient arrived at our hospital 20 min following seizure onset. By the time the patient presented to the emergency department, he was unresponsive, apnoeic and areflexic with a Glasgow Coma Scale score of 3. He had no medical history and took no medications. ECG revealed asystole. Ten minutes after presenting to the emergency room, 1 mg epinephrine was intravenously administered and the patient experienced return of spontaneous circulation (ROSC). The patient was emergently intubated. Blood test revealed haemoglobin level of 14.6 g/dL and haematocrit (Ht) level of 44.2% at arrival. No coagulation abnormalities were observed. ECG revealed ST reduction of the precordial leads and ST elevation in aVR inductionafter resuscitation. The patient was diagnosed with cardiac arrest due to acute coronary syndrome. FAST was not administered this time. A CT was ordered; however, the patient exhibited ventricular fibrillation and was moved to catheter room.
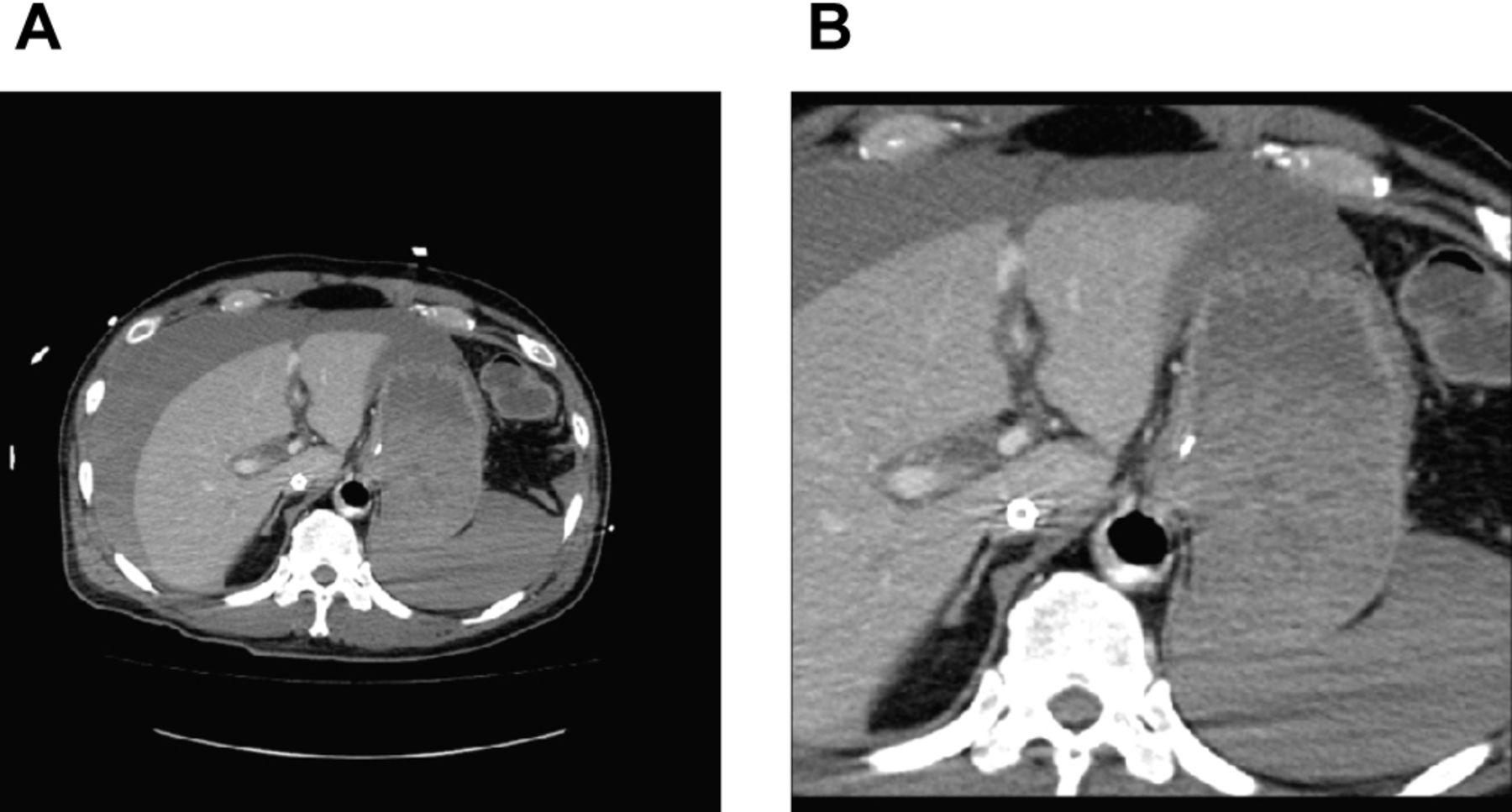
The patient underwent emergency catheter examination and percutaneous coronary angioplasty under percutaneous cardiopulmonary support (PCPS), which revealed 90% obstruction of the anterior descending branches. He exhibited ROSC and was admitted to the ICU after intra-aortic balloon pumping (IABP); subsequently, his blood pressure decreased. ECG revealed normal cardiac contractile forces outside the anterior descending branch areas. The patient continued to exhibit abdominal distention and decreasing Ht. This time we performed FAST, which revealed echo-free space around the liver and the spleen. Contrast CT examination revealed bloody ascites around the liver and the spleen, and we diagnosed intra-abdominal bleeding. A linear contrast effect was observed in the vicinity of the hepatic sickle ligament in the early phase of the contrast (figure 1). We diagnosed liver haemorrhage because the contrast effect was recognised as late contrast phase (figure 2). There was no apparent damage in the liver parenchyma. Conservative treatment was chosen because there is no indication of apparent liver parenchymal damage, and the patient’s blood pressure increased following transfusion.

(A,B) Early phase abdominal CT with contrast. A linear contrast effect is recognised near the liver sickle ligament. Abdominal fluid absorption value is approximately 50–70 HU.

{kind=link}
{kind=link}
(A,B) Late phase abdominal CT with contrast. The range of the contrast effect expands.
Outcome and follow-up
We withdrew PCPS on day 2 and IABP on day 3, with no decline in circulatory or respiratory conditions. The patient’s state of consciousness did not improve, and he was diagnosed with irreversible anoxic brain injury via head CT. Electroencephalogram results were also consistent with anoxic brain injury. Tracheotomy was performed on day 11, and the patient was discharged from the ICU on day 13.
Discussion
We report on a case of intraperitoneal bleeding due to liver injury following CPR. Although isolated cases of liver injury secondary to chest compressions appear in the literature, they are extremely rare.1 Hepatic injury is the most common CPR-related intra-abdominal complication, with an approximate incidence of 0.6%.1–7
In the present case, CPR was initiated by bystanders; however, it has been reported that there is no significant difference in the frequency of liver damage that results from CPR administered by bystander (ie, non-healthcare worker) and CPR administered by medical personnel.1 The study reported hepatic injury during CPR with decreased Ht levels noted on hospital arrival.1 However, in the present case, there was no decrease in Ht levels noted when the patient arrived at the hospital. Had our patient been considered as a CPA survivor and a trauma patient, FAST could have potentially detected liver injury earlier.
The FAST examination is easily performed in emergency and ICU settings. It is safe and able to detect peritoneal fluid in the right upper quadrant. FAST is widely considered to be the best initial imaging method, particularly for patients who are hemodynamically unstable.8
Limitations of FAST include operator-dependency and occasional failure to detect fluid volumes less than 200–500 mL.9 Focused attention on cardiac status following arrest may distract from consideration of the need for further workup. Therefore, there may be delays in diagnosing intra-abdominal haemorrhage and liver injury or they may be completely missed. Thus, the incidence of these conditions may be under-reported and patients would likely benefit from increased surveillance efforts.10
Current guidelines do not mention FAST as a form of postcardiac arrest care.11 12 Routine FAST may be appropriate for patients who are hemodynamically unstable following resuscitation because of the common language shared among clinical practice, education and research. FAST may have wide applicability to emergency medical care, particularly with respect to trauma treatment.9
Learning points
Liver trauma is a rare yet recognised complication of cardiopulmonary resuscitation that may be difficult to detect.
The focused assessment with sonography for trauma (FAST) procedure can quickly and easily diagnose liver trauma.
FAST is recommended for excluding haemoperitoneum in patients who are hemodynamically unstable following resuscitation.
Footnotes
Contributors HN and YT: planning, acquisition of data and interpretation of data. HN and MO: resources. HN and YM: supervision. HN: visualization and writing of original draft. All authors: writing, review and editing.
Competing interests None declared.
Patient consent Obtained from guardian.
Provenance and peer review Not commissioned; externally peer reviewed.