Article Text

Statistics from Altmetric.com
Description
A 67-year-old man with history of tobacco smoking presents to the emergency department with sudden onset, retrosternal chest pain radiating to the neck and associated with diaphoresis and nausea. On examination, his blood pressure was 106/42 mm Hg, pulse of 73 beat/min. He was pale, diaphoretic with IV/VI diastolic blowing murmur of unknown chronicity heard at the left sternal border. His distal pulses were faint but symmetric in all extremities. No marfanoid features. ECG showed sinus rhythm with ST segment elevation in leads aVR and V1, with widespread ST segment depression (figure 1). He underwent emergent coronary angiogram with initial diagnosis of acute coronary syndrome and impending cardiogenic shock. Angiogram revealed type-A aortic dissection extending to the aortic arch with concomitant aortic regurgitation (AR) (videos 1 and 2). On prompt recognition of aortic dissection, he was transferred to the operating room for emergent surgical repair. Intraoperative transoesophageal echocardiography (TEE) showed circumferential dissection of the proximal aorta with diastolic prolapse of a cylinder-shaped intimal flap into the left ventricle causing severe AR (videos 3–5). The dissection was successfully repaired using 30 mm Hemashield Platinum double velour woven graft (MAQUET, New Jersey, USA). Aortic valve leaflets were resuspended successfully (videos 6 and 7, figure 2) and the coronaries were intact.

Admission ECG showing sinus rhythm with ST segment elevation in leads aVR, V1 and widespread ST segment depression concerning for acute coronary syndrome
Coronary angiography in the left anterior oblique projection using 5F EXPO FL5 Catheter (Boston Scientific). The catheter tip appears in the false lumen and dives towards the origin of the left main coronary artery
Aortic root angiography using 6F Expo 145 Pig Catheter (Boston Scientific) showing a dissection flap in the proximal ascending aorta with extension to the arch. The flap prolapses into the left ventricle in diastole causing significant regurgitation of contrast material into the left ventricle
Intraoperative transoesophageal echocardiography in mid-oesophageal, aortic valve long-axis view
Intraoperative transoesophageal echocardiography with colour Doppler, in mid-oesophageal, aortic valve long-axis view demonstrating dissection of the proximal aorta with diastolic prolapse of a cylinder-shaped intimal flap into the left ventricle. The prolapsing flap prevents closure of the aortic valve leaflets causing severe aortic regurgitation
Intraoperative transoesophageal echocardiography in mid-oesophageal, aortic valve short-axis view demonstrating circumferential intimal dissection. In diastole, the dissected flap is obstructing the ostium of the left main coronary artery leading to the ECG changes seen
Postrepair, transoesophageal echocardiography in mid-oesophageal, aortic valve short-axis view
Postrepair, transoesophageal echocardiography with colour Doppler in mid-oesophageal, aortic valve short-axis view,demonstrating normal coaptation of the aortic valve leaflets with trace residual aortic regurgitation
{kind=link}
{kind=link}
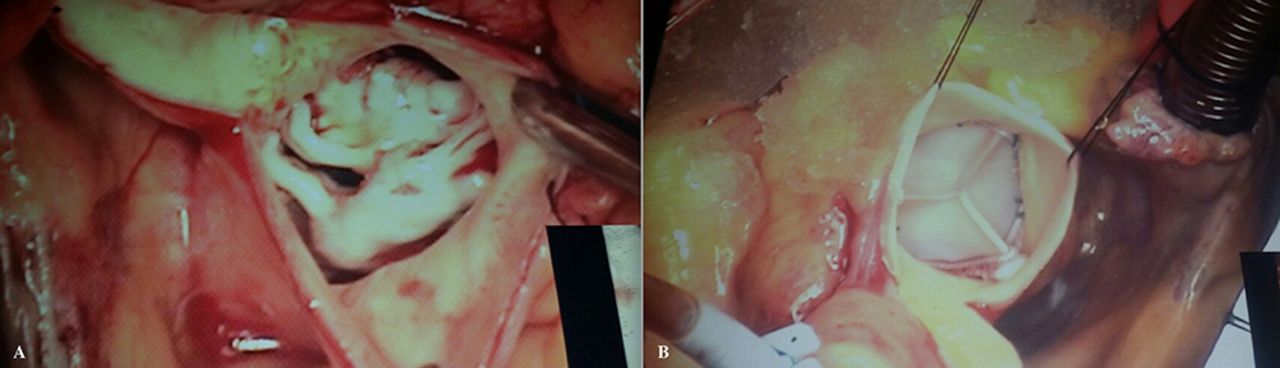
Intraoperative photograph of the aortic root and aortic valve (A) before repair and (B) after placement of the Hemashield Platinum graft and resuspension of the aortic valve leaflets
Postoperative course was unremarkable. The patient was discharged home on postoperative day 5. During outpatient follow-up at 1 week and 9 month intervals, he continued to be stable. A small-sized, non-disabling stroke was reported at his second follow-up appointment. Interval CT angiography of the aorta at 9 months showed stable postoperative changes.
Learning points
Acute Stanford type A aortic dissection is a life-threatening condition that necessitates prompt diagnosis and management. If untreated, the mortality rates have been reported as high as 60% in the first 24 hours and 90% within 3 months.1
In acute aortic dissection, the dissection flap is generally oriented along the long axis of the aorta. Circumferential intimal dissection of the ascending aorta is a rare variant. In this case, the intima undergoes circumferential tear and is separated from the aortic wall forming an intimal tube with a ‘windsock’ appearance.2 The intimal flap may telescope in a retrograde or antegrade fashion causing what is described as ‘intimo-intimal intussusception’.
A retrograde intimo-intimal intussusception and prolapse of the aortic flap into the left ventricle is a fatal form of type-A aortic dissection. The prolapsing flap could suffocate the coronary ostia and compromise aortic valve leaflets closure. This results in severe AR, rapid haemodynamic collapse and ECG changes consistent with occlusion of the left main coronary artery as expressed in our case.3
Early diagnosis and prompt operative intervention are essential for favourable clinical outcome. Unfortunately, a timely diagnosis of this type of aortic dissection is difficult since the presenting symptoms are frequently suggestive of acute coronary syndrome (ACS) and the patients are rushed to undergo coronary angiogram which potentially delays appropriate care. In our case, based on the ECG and haemodynamic findings, the impression was ACS involving the left main coronary artery with impending cardiogenic shock. All efforts were directed towards accomplishing early revascularisation which is essential for mortality benefit. However, the downstream work up revealed an aortic dissection as the primary problem instead of ACS which mandated an alternative management.
High index of suspicion for acute aortic dissection in patients presenting with acute chest pain, combined with detailed physical exam and prompt utilisation of non-invasive diagnostic imaging like echocardiography, CT or magnetic resonance angiography (if applicable from haemodynamic standpoint) are key factors in diagnosing this type of acute aortic dissection and avoiding delay in appropriate care.
Footnotes
Contributors MI wrote the manuscript and edited all videos and images. JR took care of the patient during admission and edited the manuscript. SCK performed the coronary angiogram and reviewed the manuscript. SM reviewed and edited the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.