Article Text

Statistics from Altmetric.com
Description
A 22-year-old woman presented with generalised bony pains over past 2 years. Clinical examination was unremarkable, and blood biochemistry revealed parathyroid hormone (PTH)-dependent hypercalcaemia, suggestive of primary hyperparathyroidism (albumin-corrected calcium −11 mg/dL (normal range 8.3–10.4); PTH −256 pg/mL (normal range 8–50)). Her creatinine was 0.8 mg/dL (normal range 0.6–1.2) and 25-OH vitamin D level was 31 ng/mL (30–75). She had low bone mass at distal end of radius (Z score of −2.8) and there was no evidence of renal stones. On localisation, both parathyroid scinitigraphy and ultrasound of neck localised the lesion to right inferior gland (figure 1A,B). There were no features of multiple endocrine neoplasia type 1.
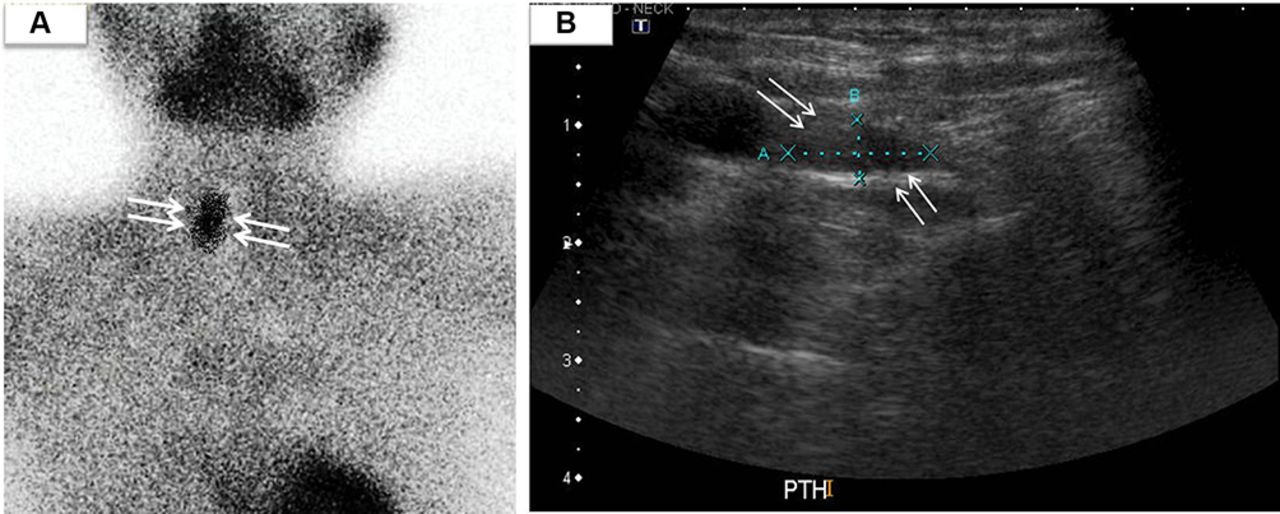
(A)Parathyroid scintigraphy displaying an adenoma at right side. (B) Ultrasound neck showing right-sided adenoma.
She underwent focused right inferior parathyroidectomy, without intraoperative PTH (IOPTH) assay. Postoperatively,however, she had persistent hyperparathyroidism, and biopsy from the excised lesion revealed thymic tissue with no parathyroid gland. A four-dimensional CT (4D CT) done subsequently helped in accurate localisation to an enlarged descended right superior parathyroid gland (figure 2). At re-exploration, an enlarged superior parathyroid gland, weighing 825 mg was identified posterior to the right recurrent laryngeal nerve (figure 3). The adenoma was seen at the lower pole of the right lobe of thyroid and was excised. Her calcium and PTH levels normalised following the surgery.

Four-dimensional CT of the neck showing parathyroid adenoma at an inferior location.

{kind=link}
{kind=link}
{kind=link}
Surgery of the neck displaying parathyroid adenoma and anteriorly located recurrent laryngeal nerve.
Involvement of multiple glands or a missed parathyroid adenoma are among the most common causes for persistent hyperparathyroidism.1 In the presence of concordant imaging, focused parathyroidectomy without IOPTH assay is an acceptable option in a resource-poor setting as in developing country like India'.2 During embryologic development, the inferior parathyroid glands migrate with the thymus and are likely to descend in the thymic region in case of mal-development. When the superior parathyroid glands (derived from the fourth pharyngeal pouch) migrate lower than the orthotopic location, they are called overly descended, but they tend to retain the important relation to the recurrent laryngeal nerve (usually located deep or dorsal to it).3 Accurate localisation of the parathyroid adenoma is essential to avert a second surgery in the absence of availability of IOPTH. Overly descended superior parathyroid glands may be lower but are deeper than inferior parathyroid adenomas. Imaging using the 4D CT scan reveals the posterior location of these glands.3
Learning points
An overly descended superior parathyroid adenoma may masquerade as an inferior lesion on planar sestamibi images.
Failure to identify the offending lesion may cause persistent hyperparathyroidism.
The utilisation of four-dimensional CT in localisation of these lesions reveals the posterior location of these tumours, and intraoperatively, they may be deeper and more posterior, but maintaining its dorsal relation to the recurrent laryngeal nerve.
Footnotes
Contributors KEC, TVP, DTA: wrote the manuscript. KEC, TVP, DTA and NT: reviewed and approved the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.