Article Text

Statistics from Altmetric.com
Description
A middle-aged African-American male with homozygous sickle cell disease presented with vaso-occlusive crisis and suffered a generalised tonic-clonic seizure while in the emergency department. He had been seizure-free for more than a decade, thus was not taking antiepileptic medications. CT head revealed diffuse cerebral oedema, effacement of the fourth ventricle and obstructive hydrocephalus (figure 1). An external ventricular drain was placed with improvement of hydrocephalus, and a repeat CT head revealed right parietal hypodensity (figure 1). MRI brain and conventional cerebral angiogram showed right parietal cerebral oedema, a large arteriovenous malformation, right internal carotid artery occlusion, moyamoya disease and basilar artery aneurysm (figure 2). The patient’s cerebral oedema and neurological examination initially improved after exchange transfusion; however, he developed acute subarachnoid haemorrhage from basilar artery aneurysm rupture and brainstem strokes causing coma. He underwent palliative extubation after discussion with family and is now deceased.

CT head shows effacement of fourth ventricle (A), diffuse cerebral oedema (B), mild obstructive hydrocephalus (C) and right parietal hypodensity (D).
{kind=link}
{kind=link}
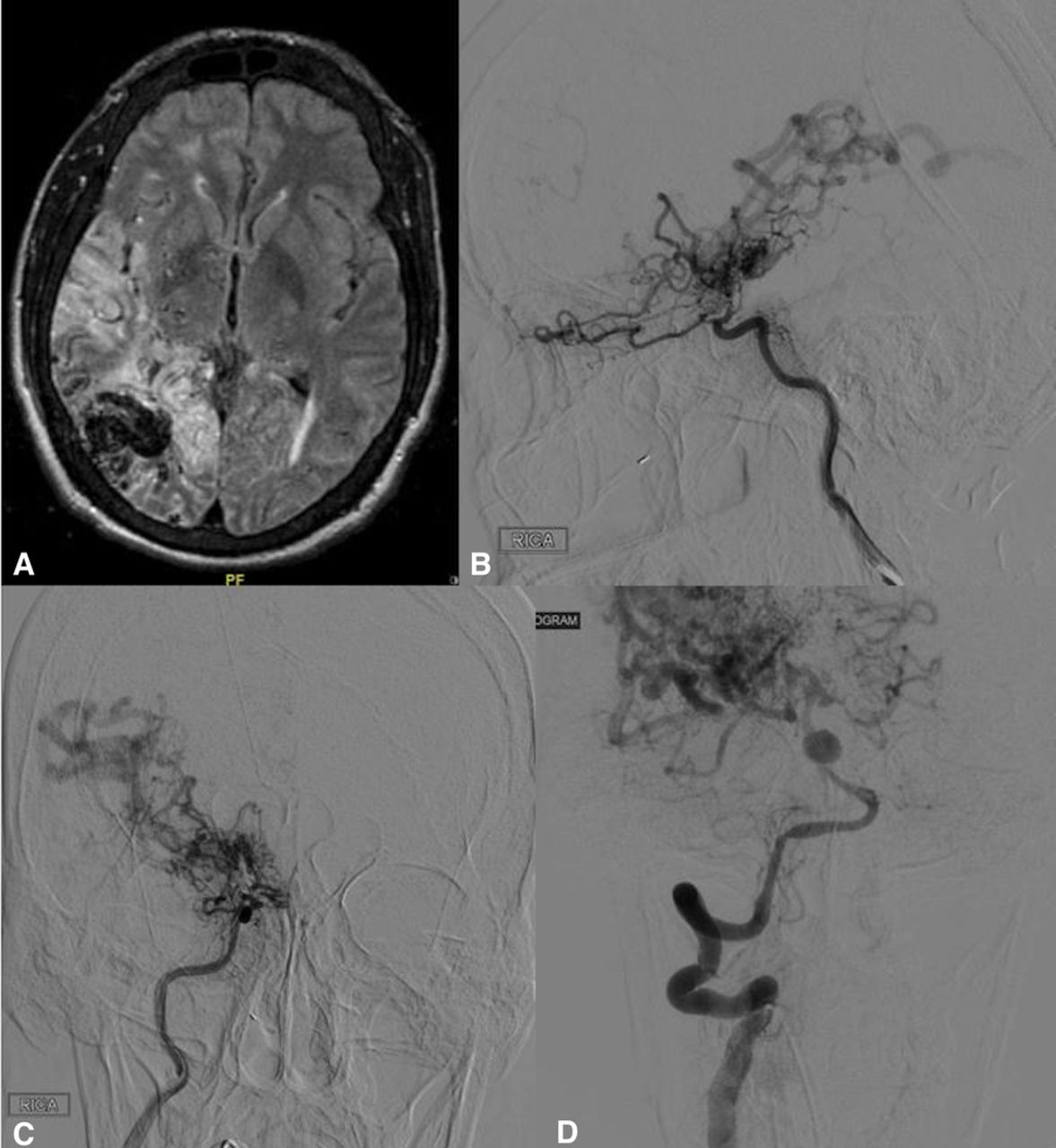
MRI brain fluid-attenuated inversion recovery (FLAIR) sequence (A) shows right parietal hyperintensity from venous hypertension-induced oedema and large arteriovenous malformation. Four vessel angiogram shows right terminal internal carotid artery occlusion and moyomoya disease distally (B and C) and basilar artery aneurysm (D).
Ischaemic strokes, haemorrhagic strokes and seizures are the most common neurological complications in patients with sickle cell disease.1 Vascular abnormalities such as arteriovenous malformations and moyomoya pattern have been described before2; however, to our knowledge, this is the first case reporting diffuse cerebral oedema complicating vaso-occlusive crisis. Vaso-occlusive crisis can precipitate venous hypertension, especially in the presence of arteriovenous malformation by obstructing the high-pressured venous system. Venous hypertension can then lead to development of cerebral oedema and hydrocephalus from obstruction of ventricular drainage. Recognising cerebral oedema as a neurological complication in patients with sickle cell disease is important, as seen in this case, and should prompt investigation for vascular abnormality.
Learning points
Chronic sickle cell disease can lead to intracranial vascular stenosis, moyamoya disease, arteriovenous malformation and aneurysm formation.
Venous hypertension and cerebral oedema can be a complication of sickle cell vaso-occlusive sickle cell crisis, especially in the presence of cerebral arteriovenous malformation.
Footnotes
Contributors MDW, TK and ED contributed to conception, planning, conduct, design and reporting. HD contributed to planning, conception and design.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.