Article Text

Statistics from Altmetric.com
Description
A 39-year-old woman was noted to have hypertension and a palpable abdominal mass at a routine general practitioner appointment. Her medical history was unremarkable.
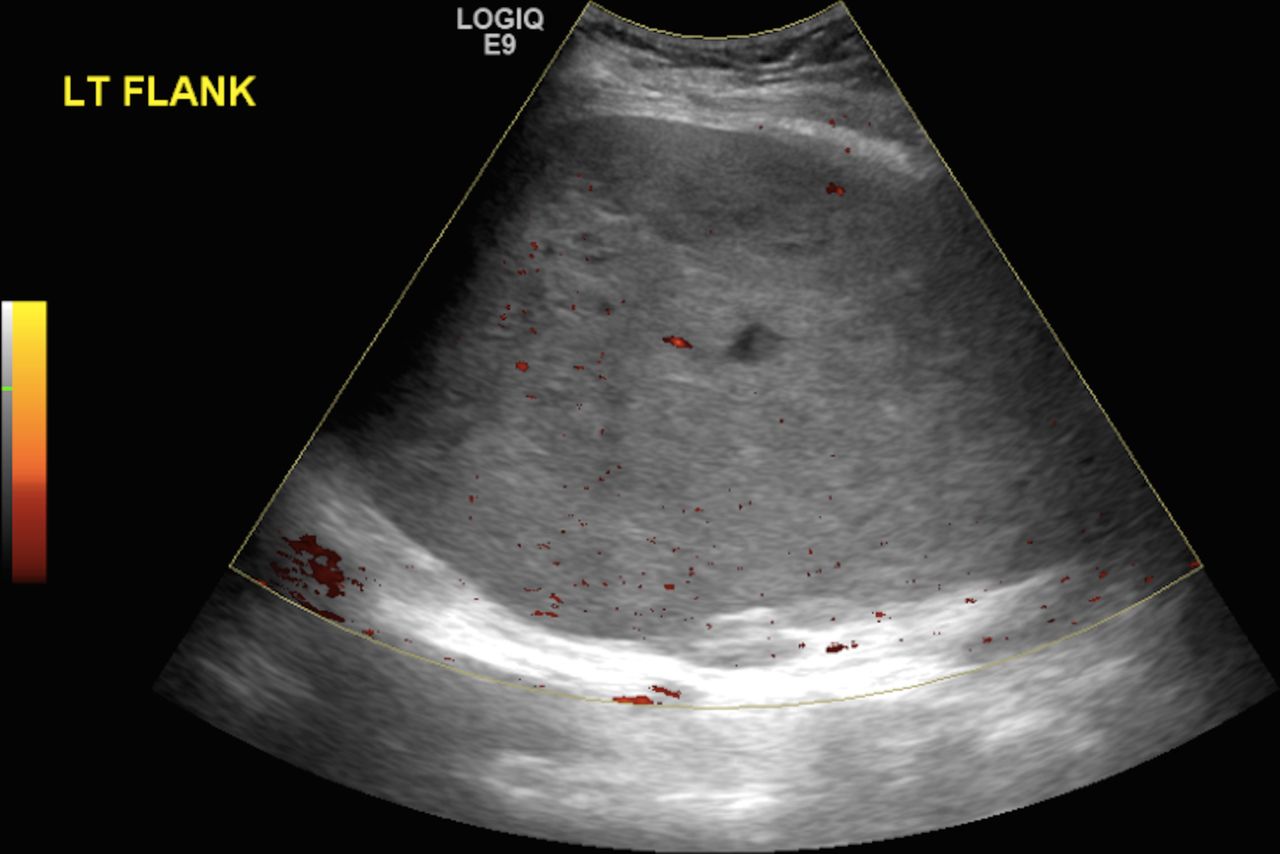
An ultrasound of the abdomen demonstrated a large mass arising from the left kidney with a smooth echotexture and patchy areas of signal heterogeneity (figure 1).

Ultrasound: there is a large mass arising from the left kidney measuring 22×13 cm. The renal mass demonstrated poor intrinsic vascularity on power Doppler assessment.
A CT scan showed an expansile hypoenhancing solid tumour arising from the mid-upper pole of the left kidney (figure 2).

Sagittal contrast enhanced CT: There is a large heterogeneous mass arising from the left kidney. The arrow points to normal renal parenchyma at the lower pole. The mid and upper poles of the left kidney are largely replaced by hypoenhancing, heterogeneous tumour.
MRI demonstrated low tumour signal on T1-weighted images and isointense signal on T2-weighted sequences (figure 3A,B). There was heterogeneous postcontrast enhancement (figure 3C). There were focal signal abnormalities consistent with haemorrhagic and cystic change (figure 3A,B).
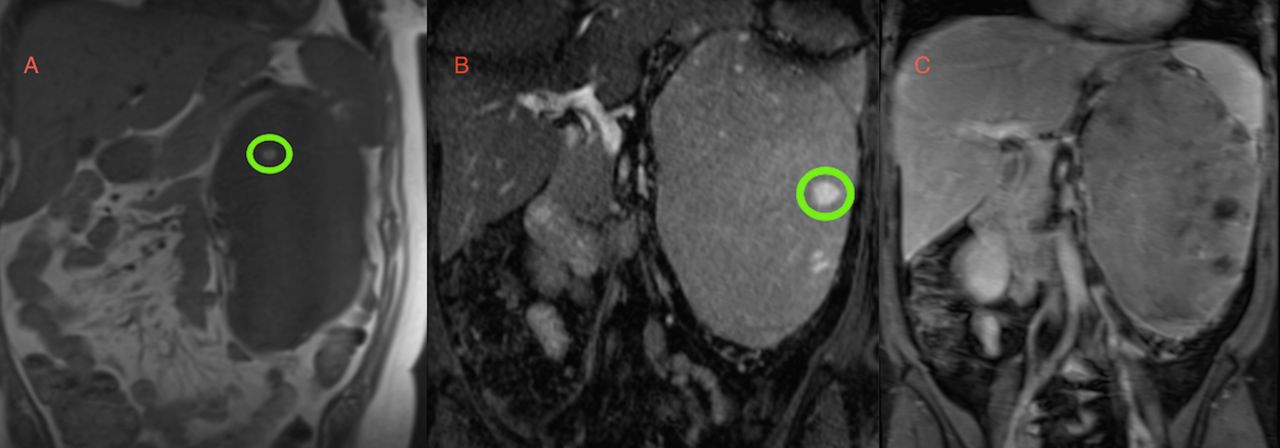
(A) Coronal T1-weighted MRI: the tumour is uniformly of low signal on T1-weighted imaging. There are regions of increased signal consistent with focal haemorrhage. (B) Coronal T2-weighted MRI: the large renal tumour is predominantly T2 isointense. The green circle highlights a region of increased signal consistent with focal cystic change. (C) Coronal MRI postgadolinium contrast: there is heterogeneous enhancement throughout the tumour.
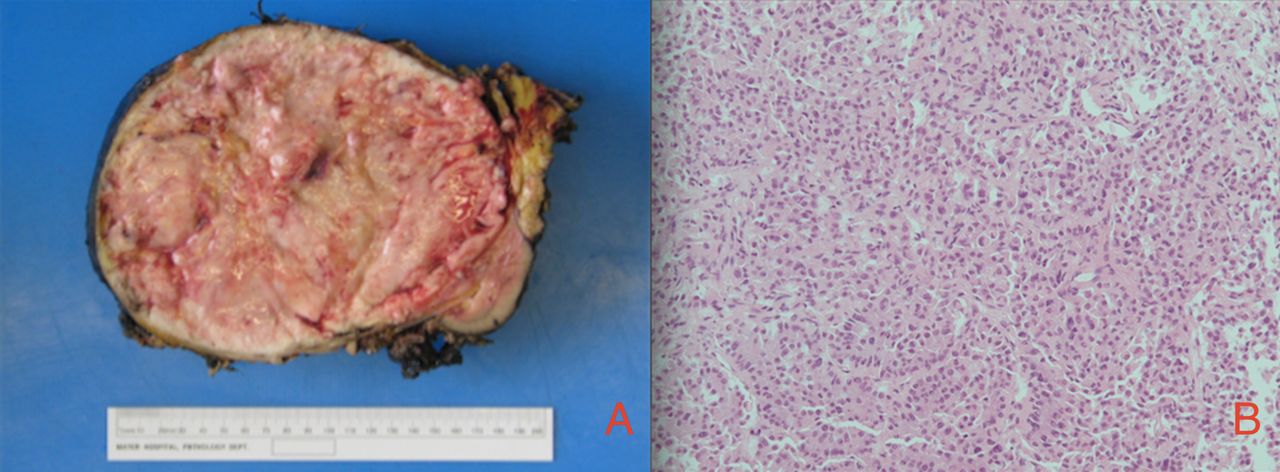
An open nephrectomy was performed (figure 4A). Histology showed a tumour composed of hyperchromatic spindle cells with an immunohistochemistry profile consistent with Wilms’ tumour (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Postnephrectomy surgical specimen. Please include description of macroscopic appearance from pathology report and the size. (B) Histology H&E slide: there are hyperchromatic spindle cells consistent with Wilms’ tumour.
Wilms’ tumour is an embryonal cancer affecting the kidneys. It is the most common solid renal mass and abdominal malignancy of childhood, with a prevalence of 1 case per 10 000 population.1 Conversely, it is very rare in adults, with an incidence rate of less than 0.2 per million per year.2 The imaging characteristics in our patient are congruent with those described in the literature for adult Wilms’ tumour.3 Histology is required for definitive diagnosis.
Learning points
Wilms’ tumour is the most common abdominal malignancy of childhood.1
Adult Wilms’ tumour is exceedingly rare but should be considered in the differential diagnosis for adult renal tumours.2
There are certain imaging characteristics that are associated with adult Wilms’ tumour. These are described in detail with corresponding images. However, histology is required for definitive diagnosis.3
Footnotes
Contributors JR: primary author. NH: performed surgery, provided clinical information. TW: assisted in surgery, provided clinical information. FB: senior author, reviewed and approved the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.