Article Text

Summary
Patients with pneumocystis pneumonia have a risk of progressing to acute respiratory failure necessitating admission to intensive care. The case described is of a patient with a newly diagnosed HIV infection presenting with pneumocystis pneumonia. Despite initiating the appropriate pharmacological treatment the patient’s clinical condition deteriorated, and required both rescue pharmacological therapy with echinocandins as well as respiratory support with extracorporeal membrane oxygenation therapy. The patient recovered well on ventilator and circulatory support despite a long weaning process complicated by sequelae common to pneumocystis pneumonia. Following initialisation of antiretroviral therapy and step-down from an intensive care setting, the patient required further prolonged hospital stay for rehabilitation and mental health support before being discharged. This case reviews the novel pharmacological therapies and respiratory support strategies used in cases of pneumocystis pneumonia, including the clinical and psychological sequelae that may follow.
- HIV/AIDS
- adult intensive care
- mechanical ventilation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Pneumonia due to Pneumocystis jirovecii (formerly carinii) is a subacute to acute pulmonary infection which develops in those who are immunosuppressed or profoundly malnourished, and is often fatal.1 Conventional therapeutic strategies against P. jirovecii revolve around early identification and severity scoring informing pharmacological therapy.2 Adjuvant therapy with corticosteroids has been found to contribute to significant reductions in mortality and need for mechanical ventilation, in particular pneumocystis pneumonia (PCP) and HIV coinfection.3 4 There are additional novel therapies that are known to be active against P. jirovecii, but these have not been subject to rigorous assessment in clinical trials, including treatment with new antifungal agents such as the echinocandin class.5
In spite of increased access to antiretroviral therapy (ART), PCP secondary to HIV infection still occurs. PCP is also increasingly recognised as a complication of immunosuppression secondary to transplantation or chemotherapy. Cases of PCP that develop acute respiratory failure requiring intensive treatment unit (ITU) admission have a poor prognosis.6 Several studies have looked at modifying optimal mechanical ventilation strategies to improve outcomes in patients admitted to ITUs with PCP.6 7 Extracorporeal membrane oxygenation (ECMO) supports gas exchange by pumping venous blood through an artificial membrane lung and returning it either into the venous (respiratory support) or arterial (cardiac support) systems.8 Respiratory ECMO has been shown to improve disability-free survival,9 and is indicated for use in cases of acute respiratory distress syndrome (ARDS) with potentially reversible causes such as infectious precipitants.10 11 Its benefit in cases of PCP requiring lung-protective ventilation has not been explored, and few cases have been reported in the literature.12–15
We present a case of a newly diagnosed patient infected with HIV who developed PCP that required ITU admission. This is an educational case because the patient did not respond to maximal conventional therapy and required both ECMO and the administration of an echinocandin rescue therapy. Few case reports exist for either therapies in HIV-related PCP, and this report hopes to contribute to the growing body of literature.
Case presentation
This 54-year-old woman presented to a large teaching hospital with a 2-week history of fevers, difficulty in breathing and a non-productive cough. This was preceded by a 3-week history of malaise, nausea, and sharp chest and back pains. There was no history of palpitations or radiation of chest pain. She described a 9-month history of unintentional weight loss of 3–4 kg, with an accompanying loss in appetite and odynophagia.
Two weeks prior to presentation, she had seen her general practitioner who had empirically diagnosed a lower urinary tract infection and prescribed a week-long course of trimethoprim, followed by another week’s course of amoxicillin/clavulanic acid. She did not improve following these treatments, and called ambulance services when she developed clinical anorexia, vomiting, fevers and difficulty in breathing. Her significant prior medical history included a depressive disorder, hypertension, hypercholesterolaemia, gastric acid-reflux disease and eczema. She owned a private business, but was not able to work for several months due to poor health. She lived with her adolescent son, and was independent in all activities of daily living. She was an ex-smoker with a 7 pack-year history. She described a recent alcohol intake history of an estimated 60 units per week for at least a few months. She did not take any illicit substances, injected or otherwise, and did not report any recent sexual contacts in the last 5 years. She described having been sexually assaulted 20 years ago, but penetrative intercourse did not occur. She did not report a history of having been investigated for sexually transmitted infections, but her last HIV test was 5 years prior and was negative. Her long-term medication included fluoxetine and lisinopril. She was not known to be allergic to any medications.
On general inspection, she appeared fatigued. She had a temperature of 36.4°C. She had a respiratory rate of 20 breaths per minute, with a capillary oxygen saturation reading of 95% on room air. Her heart rate was 78 beats per minute, with a non-invasive blood pressure of 155/85 mm Hg. Her Glasgow Comma Scale score was 15/15. Examination of her chest was completely unremarkable, and examination of the other major systems did not yield any contributory information.
A working diagnosis of a community-acquired pneumonia was established, and the patient was admitted for further investigations and management. Her initial investigations are given below. Her initial CURB-65 severity score was calculated as zero. Further investigations were conducted to look for atypical infecting organisms, including HIV testing. She was managed with appropriate fluid resuscitation and intravenous amoxicillin and clarithromycin for broad spectrum and appropriate atypical organism coverage.
On day 1 of the pre-ECMO admission period, the patient became markedly hypoxic. An arterial blood gas performed with 2 L of O2 being delivered through nasal cannulae yielded a pH 7.49, pO2 7.1 kPa, pCO2 4.0 kPa, BE 0 mmol/L and an HCO3 22.9 mmol/L. A CT pulmonary angiogram performed on the same day ruled out a pulmonary embolus as a cause of hypoxia, but confirmed a diffuse pneumonitis.
On day 2 pre-ECMO, the patient’s HIV test was reported as positive using two separate fourth-generation test kits. The clinical picture of hypoxia, cough and consolidative changes in the lung in the context of a new HIV diagnosis with a history of weight loss signifying chronicity of disease suggested a unifying diagnosis of P. jirovecii pneumonia. Oral hair leukoplakia and oral candidiasis were clinically identified on further inspection. Previous antibiotics were stopped and intravenous piperacillin/tazobactam was commenced due to evidence of clinical deterioration. Cotrimoxazole, prednisolone and fluconazole were started as treatment for presumed pneumocystis and oral candidiasis.
On day 3 pre-ECMO, CD4 quantification revealed 12 cells/mm3 consistent with an advanced, late presentation of HIV. She developed a normocytic anaemia with a serum lactate dehydrogenase (LDH) of 1431 units/L. The patient was transferred to an intensive care setting due to deteriorating ventilation resulting in type 1 respiratory failure requiring non-invasive ventilation oxygen delivery strategies. Despite being managed on non-invasive continuous positive airway pressure ventilation (set at positive end-expiratory pressure (PEEP) 10 and FiO2 65%), her capillary oxygen saturations remained between 88% and 90%.
On day 5 pre-ECMO, deteriorating oxygen requirements necessitated elective endotracheal intubation and mechanical ventilation. In accordance with evidence-based recommendations, a lung-protective ventilation strategy was employed; with tidal volumes aimed at 6 mL/kg and peak inspiratory pressures <30 mm Hg.16 Bronchoalveolar washout was performed, and an immunofluorescence test confirmed the presence of P. jirovecii.
By day 10 pre-ECMO, she had progressively worsening hypercapnia and borderline metabolic acidosis. Her serum lactate LDH continued to be raised (1349 units/L). It is recognised that P. jirovecii infection causes an increase in LDH, but on the basis of possible ineffective treatment and a worsening anaemia signalling potential haemolysis after 5 days of cotrimoxazole, second-line P. jirovecii treatment was initiated with clindamycin and primaquine. A referral to the national ECMO service was made. The patient was placed in the prone position in an attempt to improve gas exchange.17 Her ECG showed a new left bundle branch block, but a bedside transthoracic echocardiogram (TTE) showed good biventricular function. Due to the clinical deterioration, rescue therapy using caspofungin for P. jirovecii infection was initiated. Despite these measures, the patient became increasingly haemodynamically unstable and required increasing therapeutic oxygen requirements. A decision was made to place her on respiratory ECMO via bifemoral venous cannulation (23 and 25 FR), and she was retrieved to one of the five UK national commissioned ECMO centres for further management.
Investigations
The day 0 pre-ECMO admission investigations are as follows. The hospital initial laboratory tests were: haemoglobin 11.6 g/L, total white blood cell count 8.0×109 cells/L, neutrophils 6.4 (109 cells/L), lymphocytes 3.66 (109 cells/L), platelets 349×109 cells/L, bilirubin 5 μmol/L, albumin 34 g/L, globulin 41 g/L, alkaline phosphatase 181 IU/L, alanine transaminase 34 IU/L, sodium 131 mmol/L, potassium 4.1 mmol/L, blood urea nitrogen 3.2 mg/dL, creatinine 48 μmol/L and an estimated glomerular filtration rate >60. The admission chest radiograph is shown in figure 1. The admission CT pulmonary angiography is shown in figures 2 and 3.

Admission chest radiograph (posteroanterior).
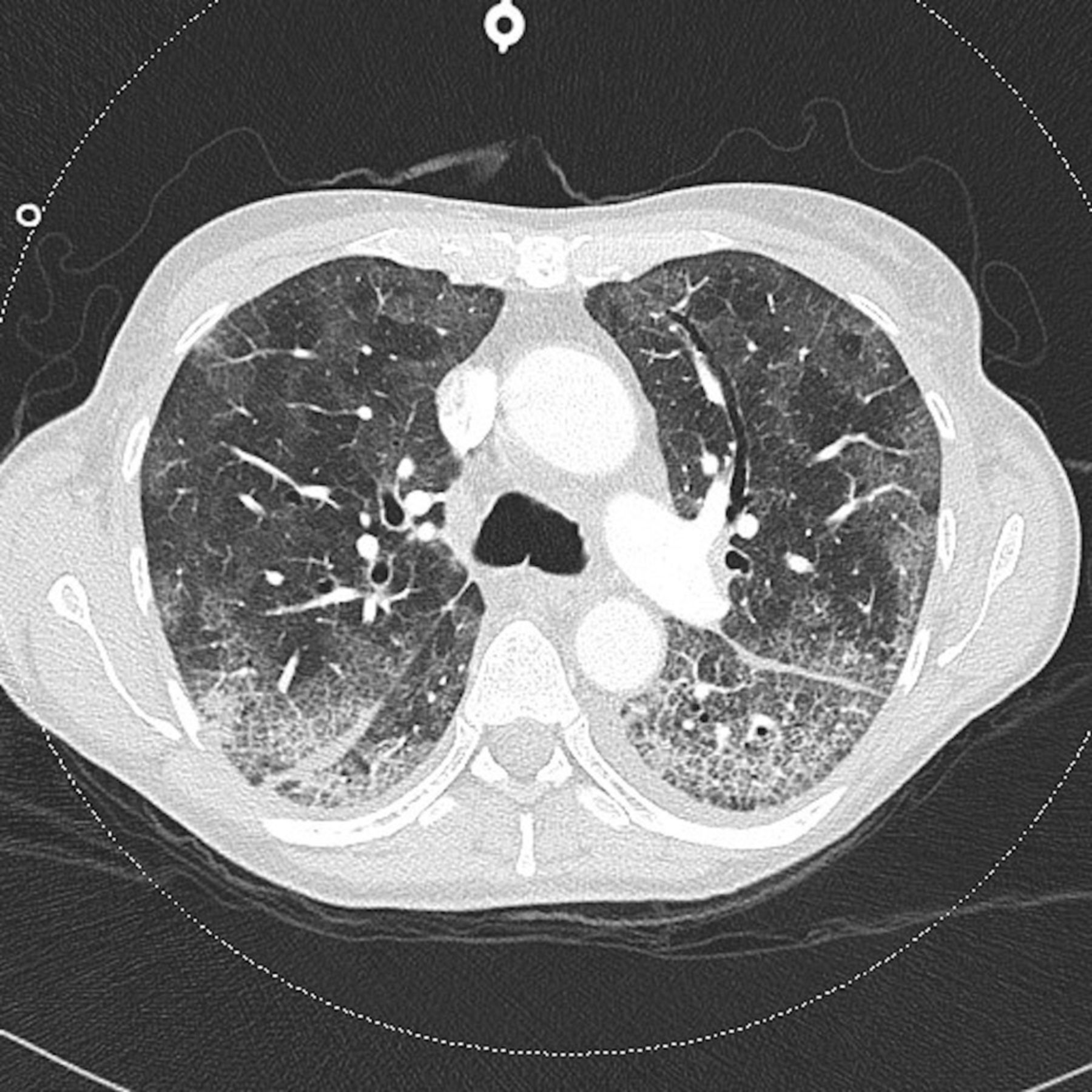
Admission CT pulmonary angiography (level of bifurcation of carina).

Admission CT pulmonary angiography (base of lungs).
The subsequent pre-ECMO and peri-ECMO admission period investigations are as follows. Initial viral screens and quantifications yielded a CD4 count of 12 cells/mm3 and an HIV viral load count of 1 075 702 copies/mL. Immunoassay or PCR screening for viral hepatitides, syphilis, cryptococcal antigen, toxoplasma and human herpesvirus-8 was unremarkable. Cytomegalovirus (CMV) DNA PCR reported 382 copies/mL. Initial beta-D-glucan antigen assays reported concentration of >523 pg/mL. Subsequent PCR from bronchoalveolar lavage samples reported P. jirovecii DNA as detected. HIV resistance investigations reported a wild-type infection fully susceptible to all ART. Periadmission (day 15) viral screens yielded a CMV DNA PCR result of 54 600 copies/mL.
Treatment
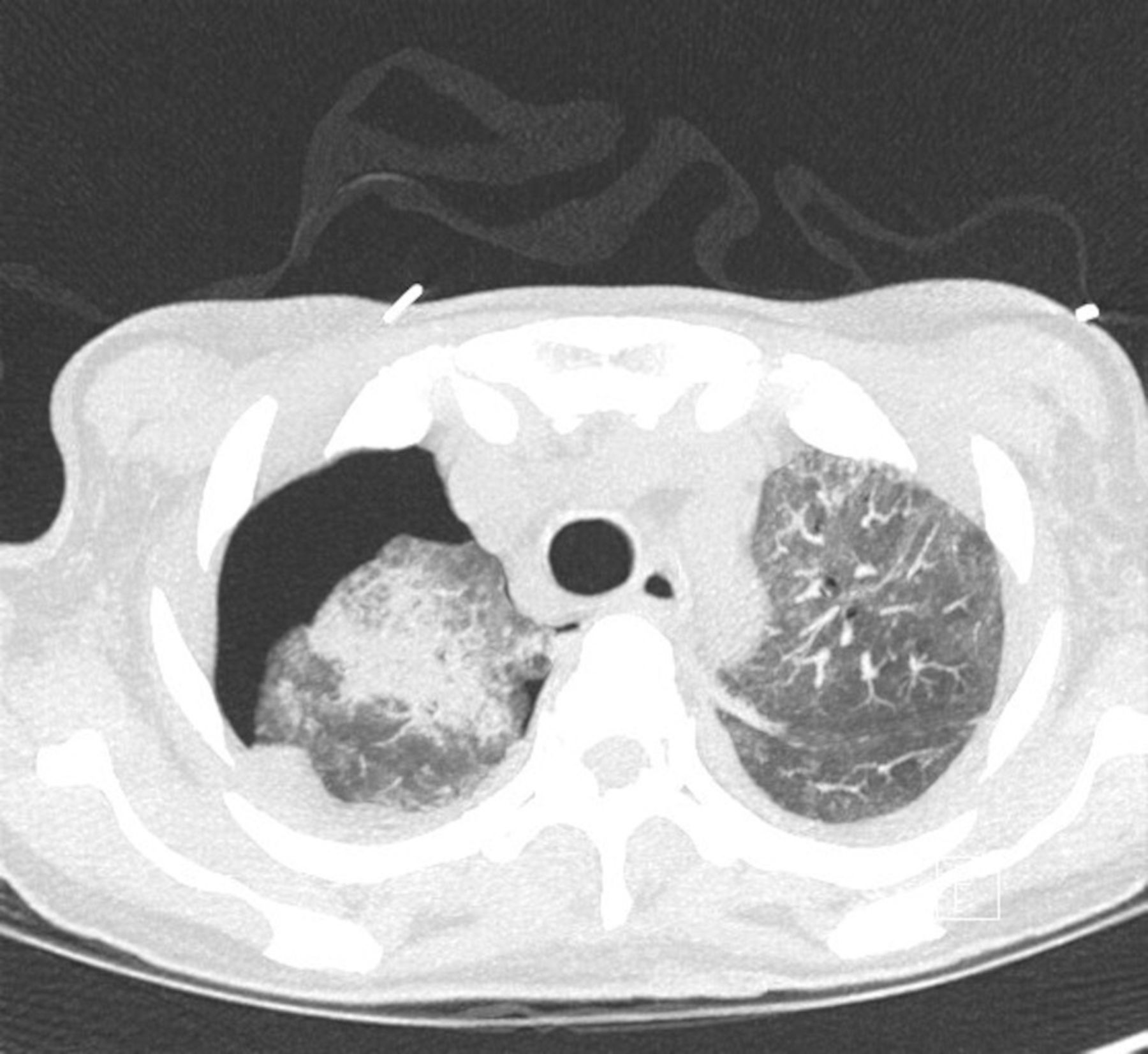
On admission to the regional ECMO centre’s ITU, the patient was placed on an ultraprotective ventilation strategy, aiming for tidal volumes of 3 mL/kg. She remained cardiovascularly unsupported and haemodynamically stable. A repeat bedside TTE showed preserved biventricular function. Her ECMO flow rate was set at 3 L/min with a sweep gas flow rate set at 1.5 L/min. A high-resolution CT employing low and high levels of PEEP to assess recruitability showed worsening consolidative and ground-glass changes throughout the lung (figures 4 and 5). Second-line and rescue treatments for PCP were continued, and intravenous methylprednisolone was added.

Post-ECMO (extracorporeal membrane oxygenation) cannulation high-resolution CT with positive end-expiratory pressure (level of bifurcation of carina).

Post-ECMO (extracorporeal membrane oxygenation) cannulation high-resolution CT with positive end-expiratory pressure (bases of lungs).
Improvement in clinical status and evidence of only single-organ failure allowed for early extubation onto high flow nasal cannulae on day 1 post-ECMO cannulation. The patient tolerated this well, and ECMO settings remained with a flow rate of 3 L/min with a sweep gas flow rate of 3.5 L/min. By ECMO day 3, the patient’s clinical condition had dramatically improved, and she began working with physiotherapy teams to complete bedside exercises with no significant compromise to her ECMO circuit flow. Due to her improving clinical condition, she began to be weaned off the ECMO circuit, made difficult by triggers of dyspnoea and anxiety. On ECMO day 8, to address ongoing ECMO weaning difficulties, she was assessed by clinical psychologist who recommended anxiolytics when it was determined that she had developed feelings of anxiety triggered by memories or thoughts of her critical illness.
On ECMO day 12, ART therapy was started. Her initial therapy included tenofovir alafenamide and emtricitabine (Descovy), and darunavir/cobivstat (Rezolsta) combination therapy. On ECMO day 15, routine investigations revealed an increasing CMV viral load for which she started on intravenous ganciclovir. On ECMO day 16, her fluoxetine dose was increased to address an ongoing adjustment disorder following her HIV diagnosis and intensive care admission on a background of an existing mood disorder. This resulted in a positive effect on her mood and engagement with rehabilitation activities.
On ECMO day 19, she was given a trial of a reduced sweep gas flow rate, resulting in a drop of peripheral oxygen saturations to 85% accompanied by an increased work of breathing despite supplemental oxygen therapy. A repeat high-resolution CT chest scan confirmed increased fibrotic and bronchiectatic changes throughout the lung, with new bilateral small pneumothoraces which were not compromising her oxygenation. She was given pulsed intravenous methylprednisolone doses for 3 days, followed by a tapering high-dose hydrocortisone maintenance therapy. On ECMO day 24, she was again trialled off sweep gas flow rate and managed to maintain good gas exchanges on nasal high-flow oxygen delivery. On ECMO day 28, sweep gas flow rates were reduced to zero, and on ECMO day 31 her ECMO cannulae were removed. This resulted in an improvement in her mood disorder as she began to work more intensively with rehabilitation teams.
Outcome and follow-up
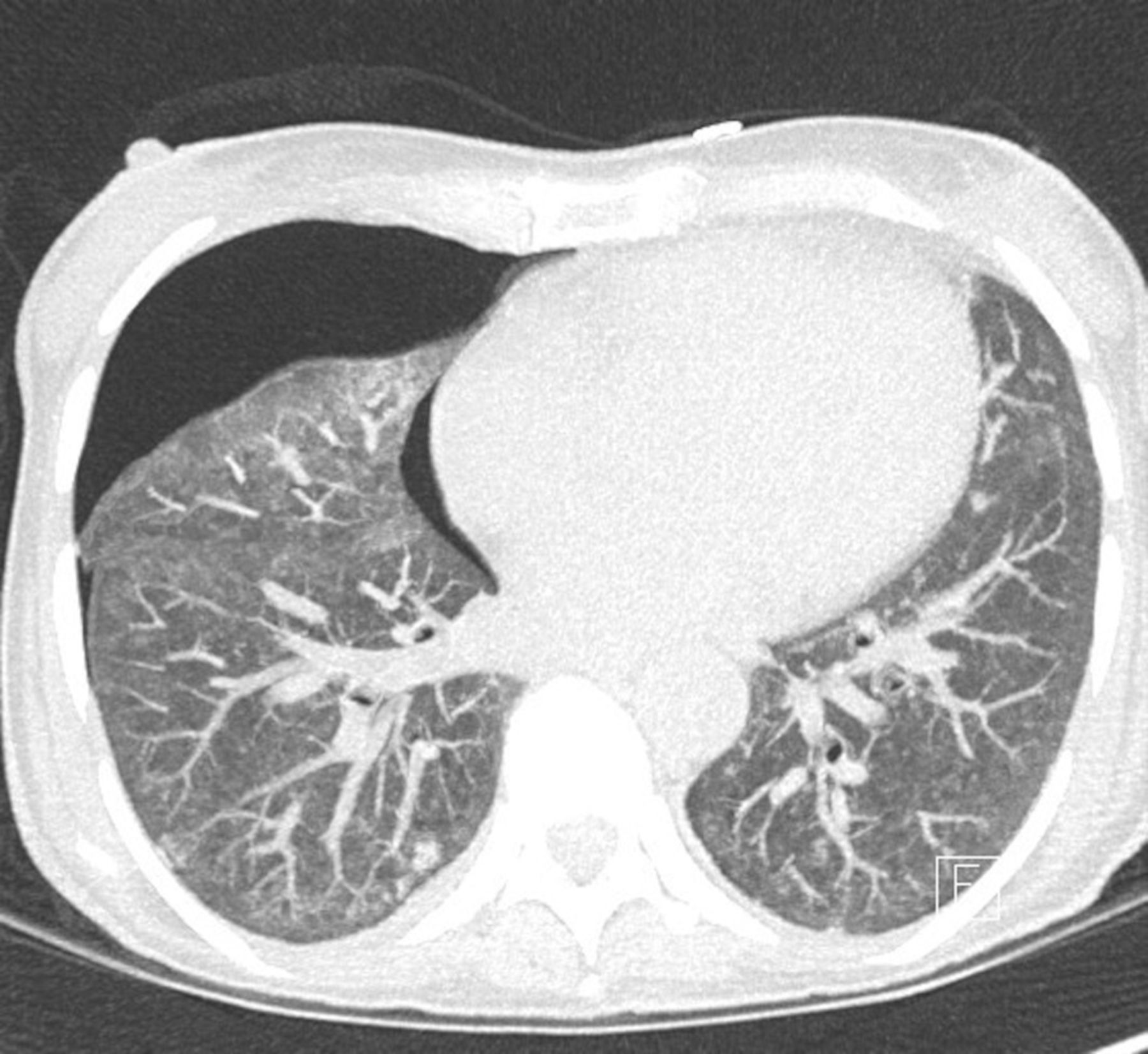
Post-ECMO decannulation, discharge planning for repatriation back to the referring hospital was initiated. However, by post-ECMO day 5, it was noted on routine X-ray imaging that her right pneumothorax had increased in size despite engaging well with rehabilitation. A repeat CT scan showed an enlarging pneumothorax, and subsequently a CT-guided chest drain was inserted (figures 6–8). Subsequent repeat X-ray imaging postdrain insertion showed good lung re-expansion.
Postchest drain insertion high-resolution CT (lung apices).

Postchest drain insertion high-resolution CT (level of bifurcation of carina).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postchest drain insertion high-resolution CT (lung bases).
Post-ECMO day 9, the patient was transferred back to the referring hospital with continuing ART, clindamycin and primaquine for PCP, gancyclovir for CMV viraemia, azithromycin for Mycobacterium avium complex prophylaxis and fluconazole for Cryptococcus spp. prophylaxis. She was stepped down to prophylactic cotrimoxazole and, as her CMV DNA was undetectable, she switched from gancyclovir to oral valgancyclovir. Repeat HIV viral parameters confirmed a CD4 count of 50 cells/mm3 and a viral load of 1555 copies/mL. The right-sided pneumothorax had resolved and the chest drain was removed 3 days after arrival to the referring hospital; however, she continued to have a persistent small left-sided pneumothorax which did not cause any clinical compromise.
The patient remained stable for 1 week before developing a recurrence of the right-sided pneumothorax. A chest drain was reinserted with minimal effect, and a decision was made after discussion with the patient to not insert further chest drains unless she developed respiratory compromise.
The patient’s prolonged period of recovery was complicated by significant weight loss and poor oral intake prompted by her deteriorating mental health. A psychiatric assessment concluded that the patient was suffering from a depressive episode in the context of an adjustment reaction to her current illness on the background of an undiagnosed personality disorder. Consequential difficulties in her ongoing management prompted detention under the UK’s Mental Health Act (MHA) for diagnosis and treatment of her underlying mental health disorder. Under these conditions, she was managed with neuroleptic medication as well as receiving nasogastric feeding for 5 weeks. As her mental state improved, the detention order under the MHA was rescinded and a complex discharge process back to her own home was arranged.
Three months post-ECMO, repeat viral parameters yielded a CD4 count of 50 cells/mm3 and a viral load of 684 copies/mL. Prior to discharge advance care decisions were made during which the patient stated a wish to not be for cardiopulmonary resuscitation, to not be transferred to an intensive care unit and to not have any further chest drains inserted. On prompting the patient for further thoughts and reflections on recent events, during numerous occasions she had stated that she would not have consented to intubation or ECMO had she known how traumatic these interventions would have been. The patient was discharged back home at 4 months post-ECMO.
Discussion
This case details the management of a newly diagnosed HIV-infected patient presenting with severe PCP requiring ITU admission for mechanical ventilation and ECMO. Treatment using second-line medications active against Pneumocystis spp. along with rescue therapy with caspofungin was used to good effect.
Pneumocystis pneumonia
P. jirovecii disease came to prominence in the last few decades following the surge of HIV cases in the 1980s/1990s.18 19 In 1981, it was first described as an opportunistic infection seen in homosexual men in America before the HIV virus had been identified.18 Prior to the introduction of ART and use of prophylactic medication, about 60% of people infected with HIV in USA, Europe and Australia were diagnosed with P. jirovecii.1 In addition, cases are seen in non-HIV immunosuppressed groups such as those receiving antitumour therapy and post-transplantation immunosuppression.20
P. jirovecii phylogenetic analysis places it within the fungal kingdom.1 19 21 Notably, they are unable to grow in fungal culture media19 and contain cholesterol instead of ergosterol in their cell wall.5 The risk of developing disease is significantly associated with CD4+ counts of <200 cells/µL and prophylaxis is given to those with counts below this figure.19
Clinical presentation usually involves dyspnoea on exertion, a dry and non-productive cough, and fever. In HIV-positive patients a significant degree of immunosuppression is required, and in those newly diagnosed with HIV these respiratory symptoms will likely have developed in the context of deteriorating health for a number of months.1 19 Radiographic signs on chest X-ray have a classical bilateral and diffuse interstitial infiltrates, as seen in figure 1 of our case. Immunofluorescence antibody stain has improved disease detection rate over traditional Gomori methenamine silver or Giemsa stains.2 20 PCR techniques are used, but these may not indicate a diseased state as P. jirovecii colonisation is increasingly found.2 20 22
Management of PCP—the role of echinocandins
First-line treatment is with cotrimoxazole (trimethoprim-sulfamethoxazole),2 19 with second-line treatment consisting of either clindamycin with primaquine, atovaquone (in mild or moderate cases) or in severe cases of treatment-resistant PCP, intravenous pentamidine which is rarely used due to its significant adverse effect profile.2 19 The antifungal class of echinocandins, in particular caspofungin, has shown activity against Pneumocystis spp. in vitro23 and in vivo24 mouse models. This is quite likely through the echinocandin’s action on (1,3)-β-D-glucan synthesis expressed by Pneumocystis spp. cell walls.5
There have been a few observational reports published looking at the effect of echinocandin therapy on PCP outcomes, but these have focused on infection related to non-HIV immunosuppression and have conflicting conclusions.25–28 There have been no well-constructed observational or interventional studies quantifying the association between caspofungin and treatment outcomes in either HIV-positive or negative cohorts.
PCP and ventilation
Severe acute respiratory failure remains a common presentation among patients with PCP.29 30 Moderate-to-severe PCPs requiring mechanical ventilatory support have a very poor prognosis, with a case fatality rate between 50% and 70%.6 Strategies in mechanically ventilated patients targeting tidal volumes of 4–6 mL/kg of ideal body weight to maintain plateau pressures less than 30 cmH2O, as per current evidence for managing patients with ARDS,16 have been shown to reduce mortality in this population (adjusted OR 0.76 per 1 mL/kg decrease, CI 0.58 to 0.99).7 Non-invasive ventilation methods offer an alternative ventilation strategy or may avoid the need for mechanical ventilation, but larger and more rigorous studies are required to assess survival benefits.31
PCP can be frequently complicated by cystic formations and pneumotoceles which place patients at higher risks of developing spontaneous or iatrogenic pneumothoraces and pneumomediastinal disease.32 Mortality in patients requiring mechanical ventilation has previously been reported between 60% and 80%.33 Hence, avoidance of positive pressure ventilation (invasive or non-invasive) through use of an extracorporeal circuit for gas exchange could theoretically reduce the risk of barotrauma and pneumothorax development.29
ECMO in PCP
The main goal in the management of ARDS is to treat the precipitating cause and support the respiratory system with lung-protective ventilation strategies.16 ECMO is a cardiopulmonary strategy that can be initiated as a rescue option in cases of ARDS where there is a severe but potentially reversible respiratory failure despite optimal lung-ventilation strategies. There are two main methods: veno-venous ECMO (VV-ECMO), which employs a central vein as a cannulation site for subsequent oxygenation and CO2 removal; and venoarterial ECMO (VA-ECMO), which involves the cannulation of a central artery and provides haemodynamic as well as respiratory support.8 The former is the modality that has been most recently evaluated for use as supportive therapy in severe acute respiratory failure.10 The Extracorporeal Life Support Organization (ELSO) guidelines recommend considering extracorporeal support based on risk of mortality (as defined by oxygen requirements and/or clinical scoring).9 34 35 ECMO can be used in these settings as rescue therapy in those who cannot maintain adequate gas transfer despite positive-pressure ventilation, or alternatively, to support lung-protective ventilation strategies in those would not tolerate the ensuing hypercapnia.8
The use of ECMO as rescue treatment of ARDS caused by infectious precipitants is becoming more common, but its use is still unclear. The CESAR (Conventional Ventilation or ECMO for Severe Adult Respiratory Failure) trial found improved mortality outcomes in patients with severe ARDS retrieved and cared for in a specialist ECMO centre, with two-thirds in each study arm being composed of infectious pneumonia-related ARDS.9 The CESAR trial did not directly compare the use of ECMO against conventional ventilation strategies, but suggested the survival benefit was likely due to cases being cared for through a specialist severe acute respiratory failure pathway. In observational cohorts and meta-analysis looking at the use of ECMO in H1N1 influenza-related ARDS, in-hospital mortality rates consistently remained high.10 11 Furthermore, with specific reference to patients presenting with immunosuppression, ELSO guidelines have listed pharmacological immunosuppression (neutrophil <400/mm3) as a relative contraindication to ECMO therapy. This may lead to avoidance of initiating ECMO treatment in patients who may otherwise benefit from this.
Literature review
To date, there are only a few case reports in the literature looking at the use of ECMO in ARDS associated with HIV-related PCP. We collate a comparative table of all published HIV-related cases of PCP that were managed with ECMO in table 1.12 13 15 36–40
Summary of reported cases of HIV-related PCP managed with ECMO.
As with the case described here, most reported cases of PCP managed with ECMO were managed using the VV modality. Our case presented with a profoundly raised HIV viral load count, likely correlating with extended length of untreated infection and an extremely low CD4 count, classifying her as a ‘late presenter’. Despite a prolonged period on ECMO compared with the other cases our patient survived hospital discharge, and this likely reflects factors involving her premorbid psychological profile. Three of the other published cases12 36 40 reported the use of echinocandin therapy; with De Rosa et al reporting the use of caspofungin as rescue therapy as in our case, Gutermann et al describing the use of caspofungin in the treatment of comorbid invasive Aspergillus spp. and Horikita et al reporting the use of micafungin as an apparent rescue therapy.
American41 and British42 guidance on the management of opportunistic infections in patients with HIV recommends that the optimal timing of ART initiation in those with PCP should be early, following the diagnosis. A randomised controlled trial comparing early initiation (within 14 days) with deferred treatment (given after treatment completion for any opportunistic infection present; approximately 6 weeks) showed reduced time to AIDS progression or death (HR 0.53; 95% CI 0.30 to 0.92).43 The development of an immune reconstitution inflammatory syndrome (IRIS) is an important factor contributing to the timing of initiating ART therapy. Although cases of IRIS post-ART initiation in PCP have been detailed,44 the reported incidence is low. In the case presented here, given the level of immunosuppression and the severity of the PCP, it was safest to establish treatment for 2 weeks and use this period to monitor for the emergence of any other opportunistic infections, including those more commonly associated with an IRIS, before initiating ART. This patient had not deteriorated significantly after commencing ART and this is consistent with her CD4 count, which had very slowly increased. In other patients, steep rises in CD4 counts can occur shortly after initiating ART, and it is these patients who often deteriorate clinically.
The success of ECMO therapy in our case allowed for extubation from mechanical ventilation while on ECMO. The use of ECMO in awake and self-ventilating patients with respiratory failure is an increasingly more commonly seen treatment strategy (‘awake’ ECMO).45 46 In the case of our patient with PCP, the benefits of awake ECMO included the liberation from invasive mechanical ventilation and subsequent protection from ventilation-associated complications (reduced risk of barotrauma and reduced risk of acquired ITU-associated deconditioning) and therapy-orientated factors (reduction in delirium and improved rehabilitation potential).45 To our knowledge, the patient presented in this case was the first PCP case to be managed with an ‘awake’ ECMO strategy. However, despite the physiological benefit seen in ECMO, the patient presented in this case ultimately developed negative psychological sequelae that likely impeded her overall clinical improvement. It must be stated that the long-term negative effects that ECMO may have on clinical outcomes have been documented previously. Indicators of psychological morbidity including functional quality-of-life scores47 48 and return to work49 were all reduced in patients who had undergone ECMO.
Learning points
Extracorporeal membrane oxygenation (ECMO) represents a viable therapeutic strategy for patients presenting with pneumocystis pneumonia (PCP)-associated acute respiratory distress syndrome. ECMO allows facilitation of ultra-lung protective ventilation strategies and awake ECMO may provide further ventilation, rehabilitation and psychological benefits. The selection of patients for veno-venous ECMO remains difficult, particularly in immunocompromised patients, and further work should be done to investigate the benefit of ECMO therapy in this patient group.
Caspofungin therapy may provide clinical benefits in the management of patients with PCP, particularly in cases where first-line therapy is not tolerated. Randomised controlled trials assessing their effectiveness are required.
ECMO rescue therapy can be a very traumatic experience for patients both physiologically and psychologically. Considering premorbid psychological factors and long-term quality-of-life outcomes is important for clinicians when assessing candidates for ECMO.
References
Footnotes
Contributors NL conceptualised the project, initiated and completed data collection, drafted initial and final versions of manuscripts, and provided final input to accepted version. DL and BP contributed patient data and provided input to the initial and final manuscripts. SL provided patient data, acquired patient consent for publication, and contributed to the initial and final manuscripts.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.