Article Text

Statistics from Altmetric.com
Description
A 7-year-old South Asian boy was evaluated in a district general child assessment unit following a 4-week history of daily fevers with associated pain and swelling in the thumb and middle finger phalanges of the right hand. There was no history of cough, weight loss, night sweats or trauma. On examination, he appeared well with no anaemia or jaundice. There was a spindle-shaped deformity of the right thumb and middle finger, with concomitant non-tender right axillary lymphadenopathy. No other joints were affected. The rest of the physical examination was unremarkable.
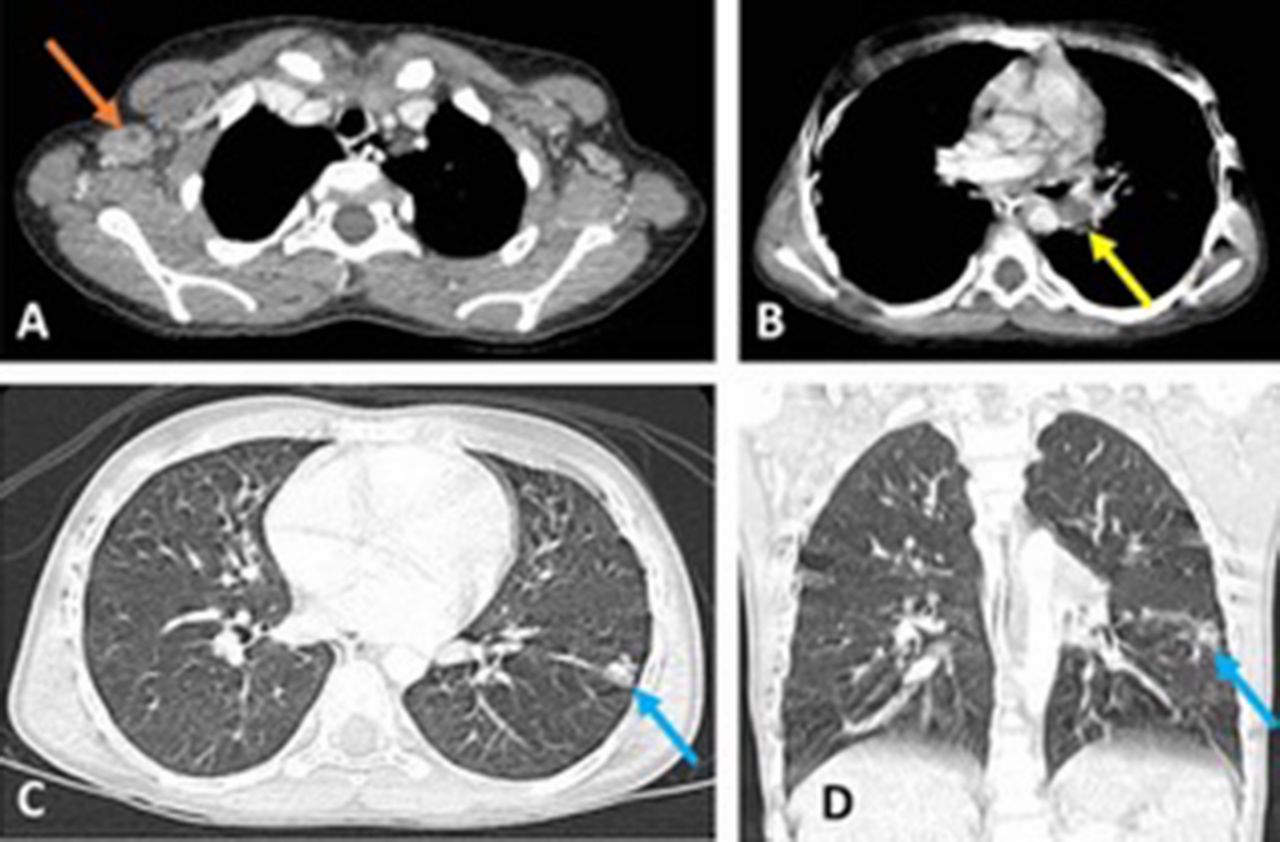
Radiographs of the affected fingers demonstrated fusiform soft tissue swelling (Figure 1A) with smooth periosteal reaction (Figure 1B). Subsequent CT of the thorax demonstrated necrotic axillary (Figure 2A) and hilar lymphadenopathy (Figure 2B) with ‘tree-in-bud’ change in the superior segment of the left lower lobe (Figure 1C).
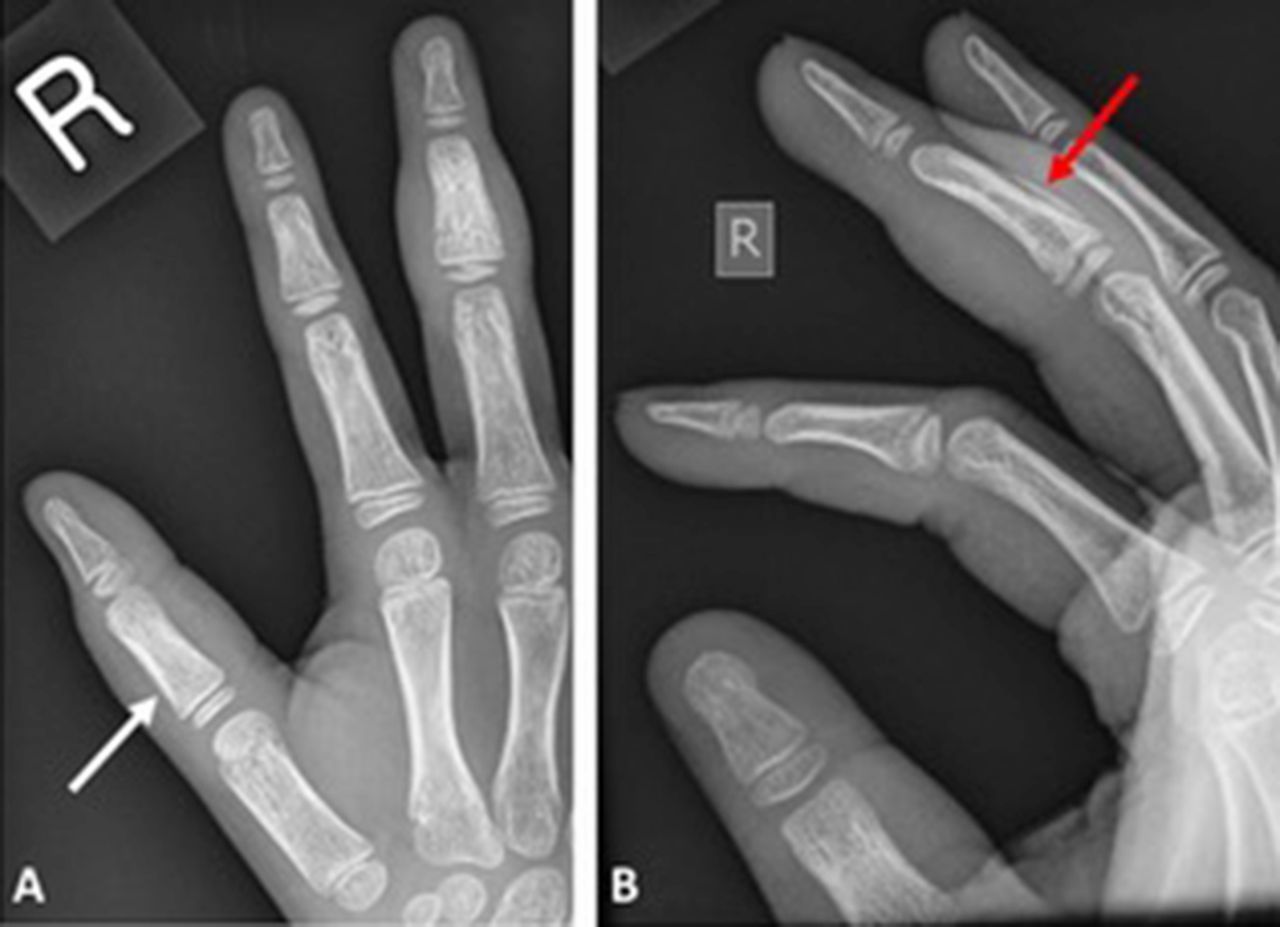
Cropped radiographs of the right hand. (A) Dorsoplantar projection demonstrates relative sclerosis and osseous expansion of the intermediate phalanx of the middle finger with associated fusiform soft tissue swelling and unilamellar smooth periosteal reaction of the diaphysis, best seen on the (B) lateral view (red arrows). The proximal phalanx of the thumb is affected to lesser extent with faint periosteal reaction (white arrow). Given the confirmed diagnosis of tuberculosis, radiological appearances are consistent with spina ventosa (short bone expanded with air) or tuberculous dactylitis.
{kind=link}
{kind=link}
CT of the thorax. Selected soft tissue window axial slice (A) demonstrates a large axillary lymph node (22×13 mm) with an eccentric area of low attenuation consistent with necrosis (orange arrow). A more inferior axial slice (B) demonstrates a 15-mm non-enhancing low attenuation necrotic lymph node (yellow arrow). A small area of ‘tree-in-bud’ change in the apical segment of the left lower lobe is consistent with a Ghon focus (blue arrow), as seen on the lung window (C) axial slice and (D) coronal reconstruction. Radiological appearances are consistent with pulmonary tuberculosis.
A Mantoux test (protein purified derivative) was positive with an induration of 30 mm. QuantiFERON (interferon-γ release assay) was also positive. Haemoglobinopathy screen was negative. A biopsy of the affected phalanges revealed granulomatous inflammation with the presence of necrosis and giant cells; Mycobacterium tuberculosis PCR was positive. The diagnosis of tuberculous dactylitis and pulmonary tuberculosis were made given the constellation of clinical, radiological and laboratory findings: he was commenced on an appropriate antituberculosis drug regimen.
Learning points
Dactylitis, diffuse fusiform swelling of a digit(s), has a wide differential diagnosis including:1
infectious (osteomyelitis, syphilitic and tuberculous (spina ventosa));
haematological (sickle cell disease and leukaemia);
arthropathic (psoriatic, hyperparathyroidism, gout and sarcoidosis).
Reference
Footnotes
Contributors AF: involved in the clinical care of the patient; obtained informed consent; co-wrote the manuscript text. GT: involved in the clinical care of the patient; reviewed the manuscript text. MP: extracted, reformatted and labelled all the imaging; wrote all the figure legends; co-wrote the manuscript text.
Competing interests None declared.
Patient consent Obtained from guardian.
Provenance and peer review Not commissioned; externally peer reviewed.