Article Text

Statistics from Altmetric.com
Description
A 70-year-old woman with controlled type 2 diabetes mellitus and hypertension presented for evaluation of chronic abdominal discomfort. An incidental 3.2×3.5×3 cm left adrenal mass was identified on CT. Physical examination revealed obesity stage 2 without a Cushingoid appearance and controlled hypertension with a regular heart rate. Biochemical evaluations for Cushing syndrome, primary aldosteronism and pheochromocytoma were negative. A 1-year follow-up CT of the adrenal glands with washout showed a larger left-sided adrenal mass, measuring 4.3x3.4x3 cm (figure 1A). The attenuation values of the mass were indeterminate: non-contrast, 15 Hounsfield unit (HU); portal venous, 70 HU; delayed, 42 HU; absolute washout, 51%. MRI of the abdomen confirmed the left adrenal mass (figure 1B,C). Given the rapidly increasing size, malignancy was suspected and a whole-body positron emission tomography/CT scan using 18F-fluorodeoxyglucose (18F-FDG) was performed, which demonstrated (figure 1D,E) an 18F-FDG avid adrenal mass (standardized uptake values (SUV)max: 6.16) with increased activity compared with the liver background (SUVmax: 2.4). Adrenal incidentalomas are lesions that are detected on imaging performed during the evaluation of non-adrenal disease, with a prevalence of ~4%–10% of all scans.1 2 Patients with an incidentaloma should undergo evaluation for Cushing syndrome or autonomous cortisol secretion, pheochromocytoma, primary aldosteronism if hypertensive or a malignant tumour (particularly if size >4 cm).3 Non-functional adrenal adenomas rarely show increased 18F-FDG activity; their SUV should be compared with the average 18F-FDG uptake by the liver. Given the size of the adrenal mass and the increased 18F-FDG uptake, a left laparoscopic adrenalectomy was performed to rule out adrenocortical carcinoma. Microscopic examination showed mainly clear cell pattern with a focal eosinophilic component, and a Weiss score of zero, consistent with a benign adrenocortical adenoma (figure 2). The patient did well after surgery.

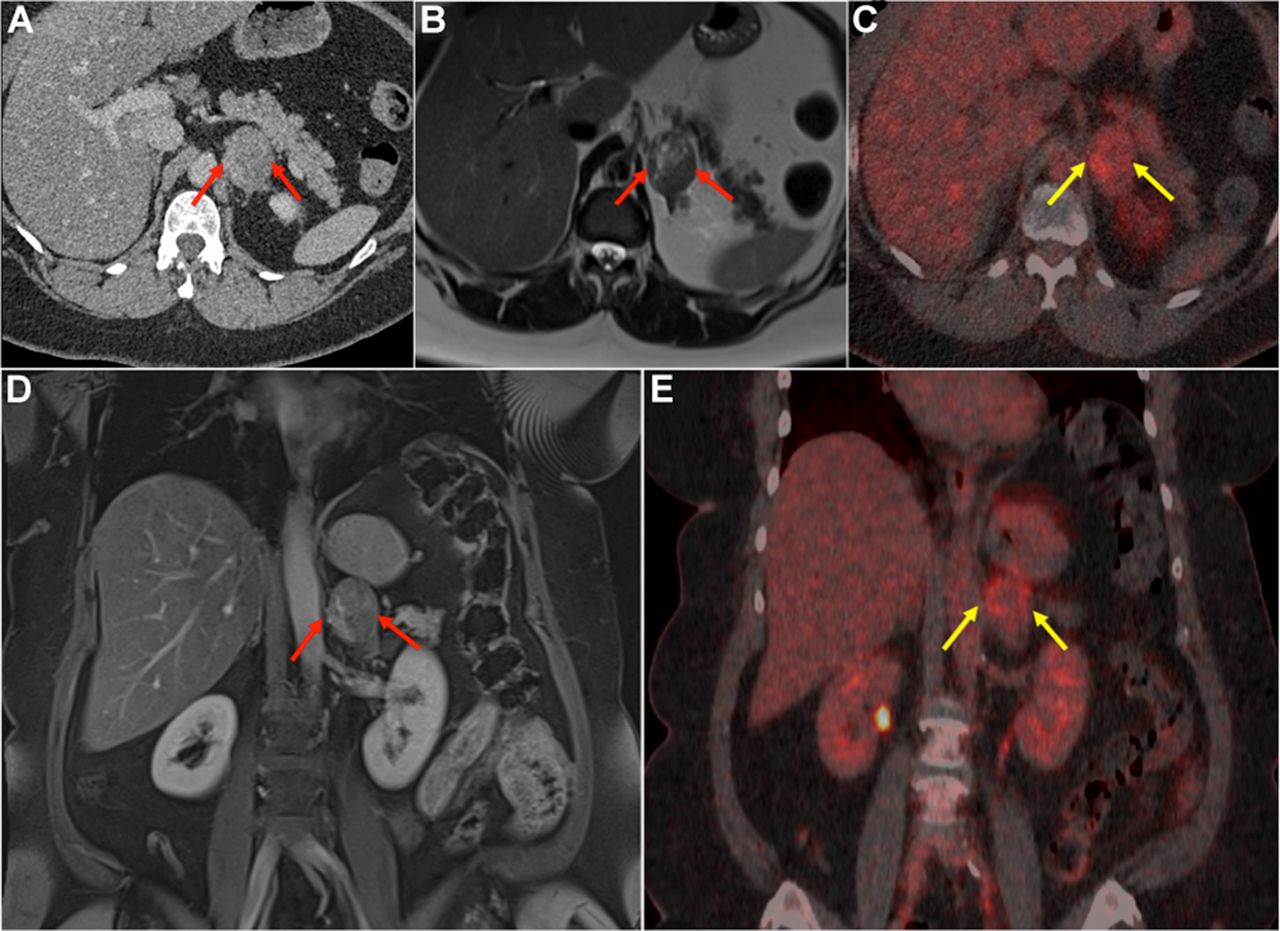
(A) Axial postcontrast CT image of the abdomen showing (arrows) a nodular mass in the left adrenal gland measuring 4.3x3.4x3 cm with low attenuation (non-contrast HU: 15). (B) Axial T2-weighted MR-image of the abdomen showing the left adrenal mass (arrows) with central areas of increased T2 signal. (C) Coronal fat suppressed contrast enhanced T1-weighted MR-image of the abdomen showing (arrows) the left adrenal mass with areas of contrast enhancement. (D) and (E) Axial and coronal fused 18F-FDG PET/CT images of the abdomen demonstrating (arrows) a hypermetabolic left adrenal mass with increased activity (SUVmax: 6.16) compared with the liver background (SUVmax: 2.4). HU, Hounsfield unit; PET, positron emission tomography.
{kind=link}
{kind=link}
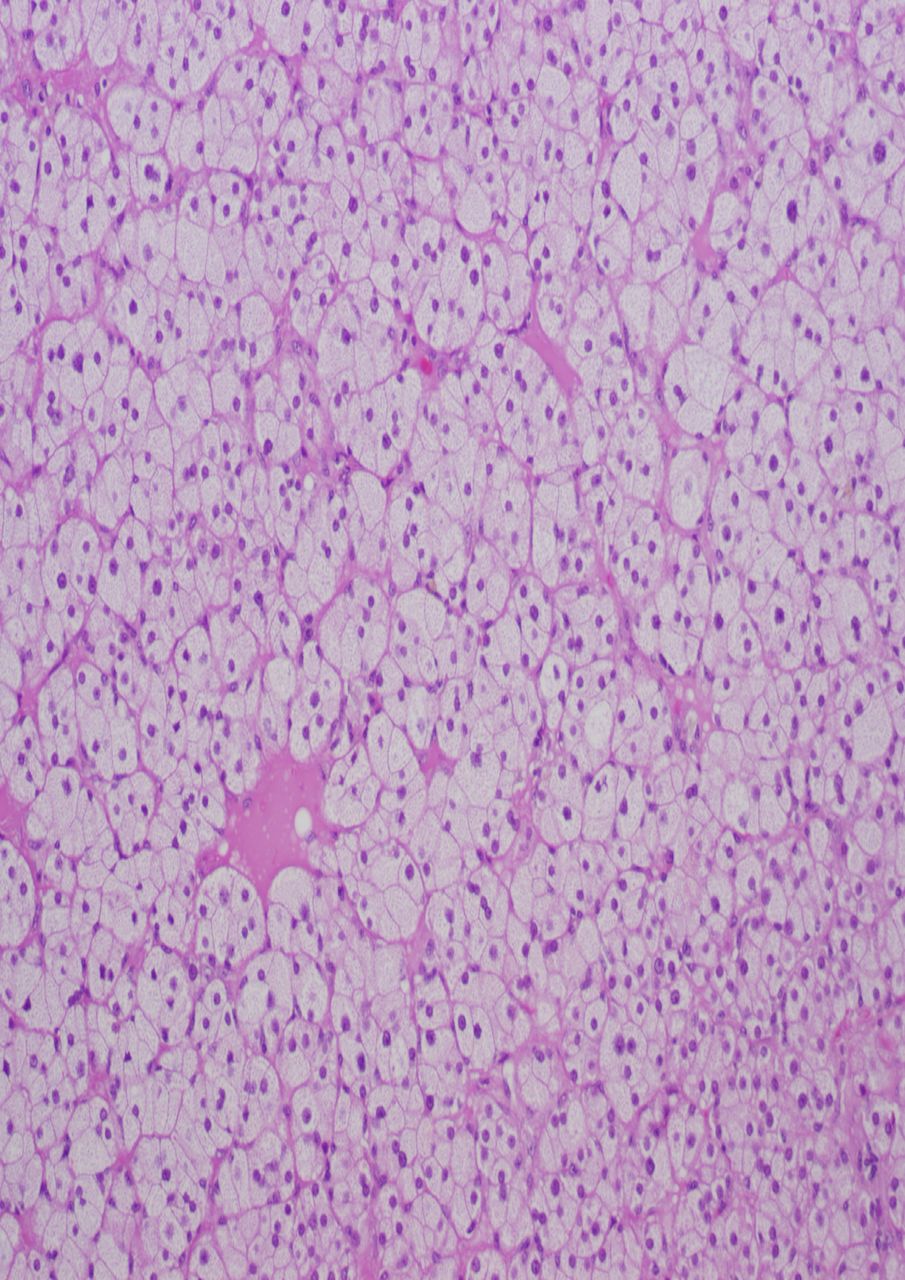
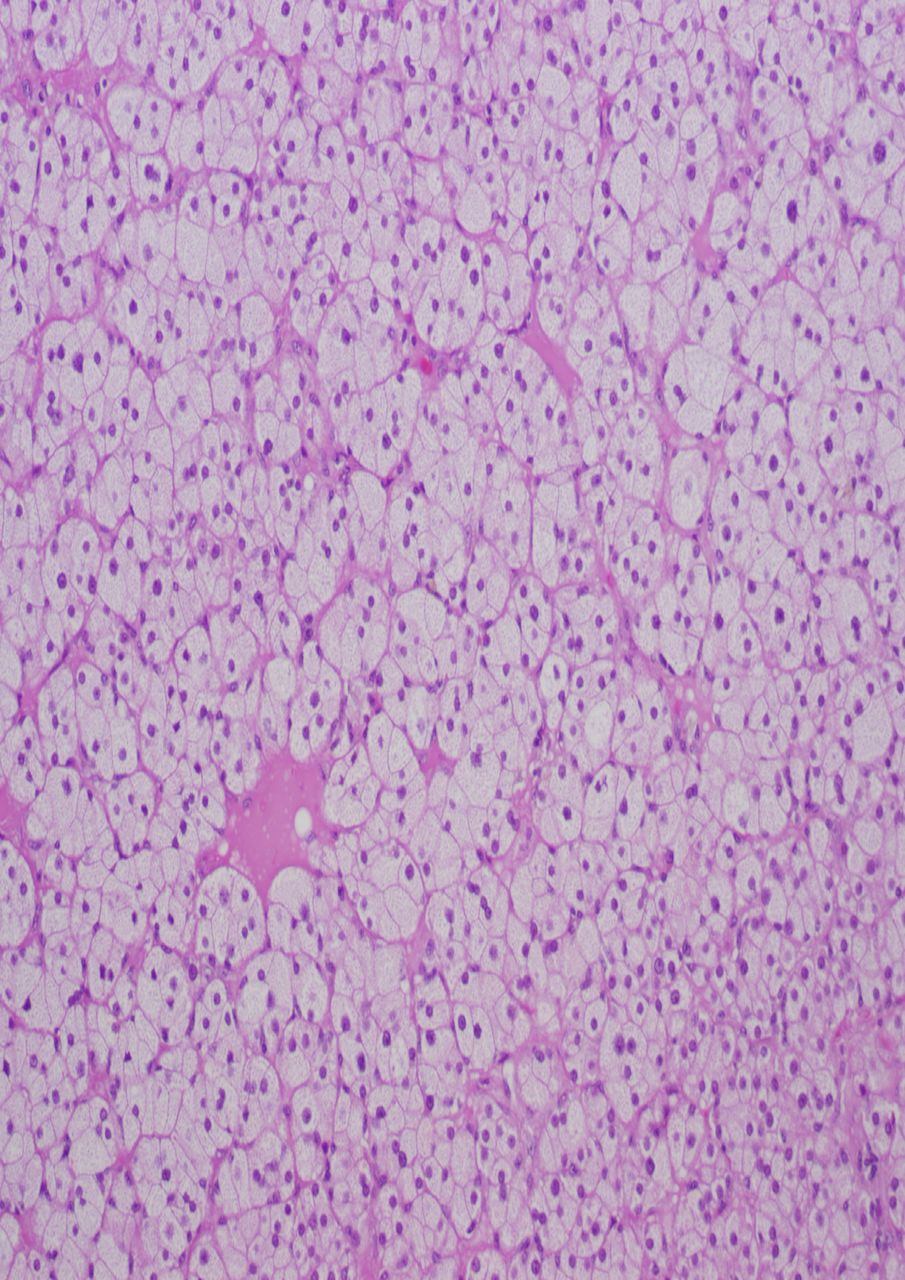
Microscopic examination showed mainly clear cell pattern with a focal eosinophilic component, consistent with a benign adrenocortical adenoma.
Learning points
Adrenal incidentalomas are lesions that are detected on imaging performed during the evaluation of non-adrenal disease, with a prevalence of ~4%–10%.
Non-functional adrenal adenomas rarely show increased 18F-FDG activity; their SUV should be compared with the average 18F-FDG uptake by the liver.
Footnotes
Contributors FH-S, GZP, CAS and JB were involved in the planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.