Article Text

Statistics from Altmetric.com
Description
A man aged 24 years presented with acute abdominal pain since 2 days. His past medical history was unremarkable. On physical examination, the abdomen was tender, soft and tympanic to percussion, with absent bowel sounds. CT of the abdomen revealed imaging signs indicating mechanical small bowel obstruction (SBO) related to ileal wall thickening (figure 1A) and to the presence of an alimentary fragment (an olive with its stone, one of the favourite foods of the patient) (figure 1A). The nature of the foreign body causing the SBO was suspected by the detailed history taking of the patient’s alimentary habits. To confirm this diagnosis, a CT acquisition (figure 1B) of fresh olives (figure 1C) was made and the picture was compared with the patient images.
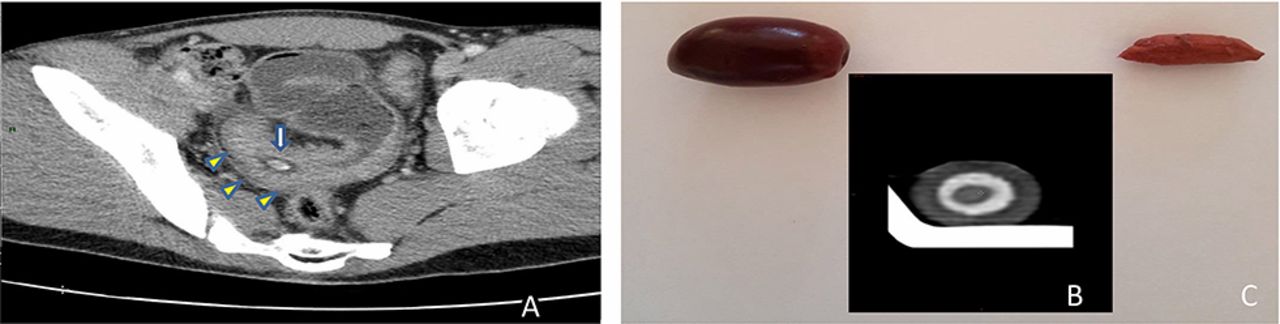
(A) Pelvic small bowel dilated loop with an ileal wall thickening (Crohn’s disease, yellow arrow) and entrapment of an olive with its stone (white arrow). (B) CT acquisition of a black fresh olive in a pot. (C) Fresh olive and its kernel.
After conservative medical management, the patient completely recovered and underwent an ileocolonoscopy (figure 2A and B) with biopsy, which showed Crohn’s disease of the terminal ileum. Usually, inflammatory bowel disease presents with diarrhoea, bloody stools, abdominal pain and weight loss but occlusion due to foreign body is rare. Most ingested foreign bodies are conveyed safely through the gastrointestinal tract and are occasionally complicated by bowel obstruction. This complication is very rare with olives.1 This is also the first time that CT acquisition of a fresh olive has been compared with patient images.

{kind=link}
{kind=link}
(A) Ileoscopy showing narrowing of the terminal ileum and fibrotic aspect with scarred mucosa. Presence of a fistula orifice in the lower left part of the figure (arrow). (B) Ileoscopy showing mild erythema, single superficial ulcer and presence of blood (due to the contact with the endoscope).
Learning points
Small bowel obstruction (SBO) related to olive kernel is rare and when a patient comes with SBO, physician should always look for an underlying disease (eg, inflammatory bowel disease, cancer, lymphoma).
Footnotes
Contributors Professor ED helped us in understanding the CT acquisition. Dr YH took care of the patient and managed this patient. They contributed equally to the writing of this paper. Dr OD carried out the colonoscopy and is the gastroenterologist now taking care of the patient.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.