Article Text

Statistics from Altmetric.com
Description
A 77-year-old Caucasian man presented to the oncology service with de novo v-raf murine sarcoma viral oncogene homolog B (BRAF), wild-type metastatic melanoma and widespread disease involving; subcutaneous fat, lymph nodes, bone and spleen with no history of autoimmunity. At diagnosis, the spleen was measured within normal limits on CT. In November 2013, he commenced treatment on a phase-III randomised double-blinded clinical trial (CA209-067) and received combination checkpoint inhibitor therapy with ipilimumab and nivolumab.
Radiological mixed response was observed after three months, with a partial response in all target lesions (RECIST V.1.1 criteria) but an increase in the size of the non-target splenic metastasis consistent with pseudoprogression. In conjunction, splenic enlargement was demonstrated (figure 1).
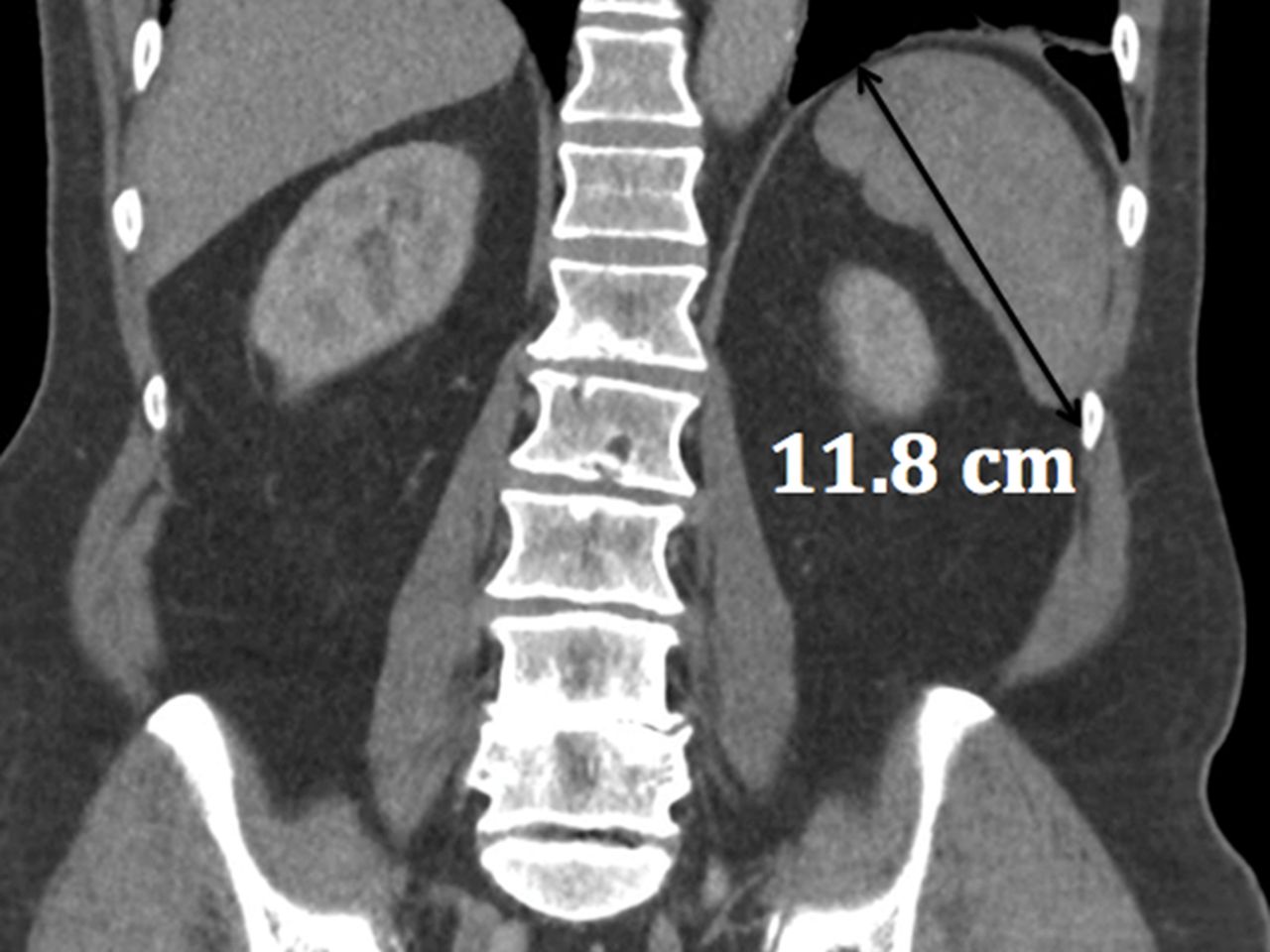
Subsequent restaging coronal abdominopelvic CT demonstrating an increased splenic length of 11.8 cm.
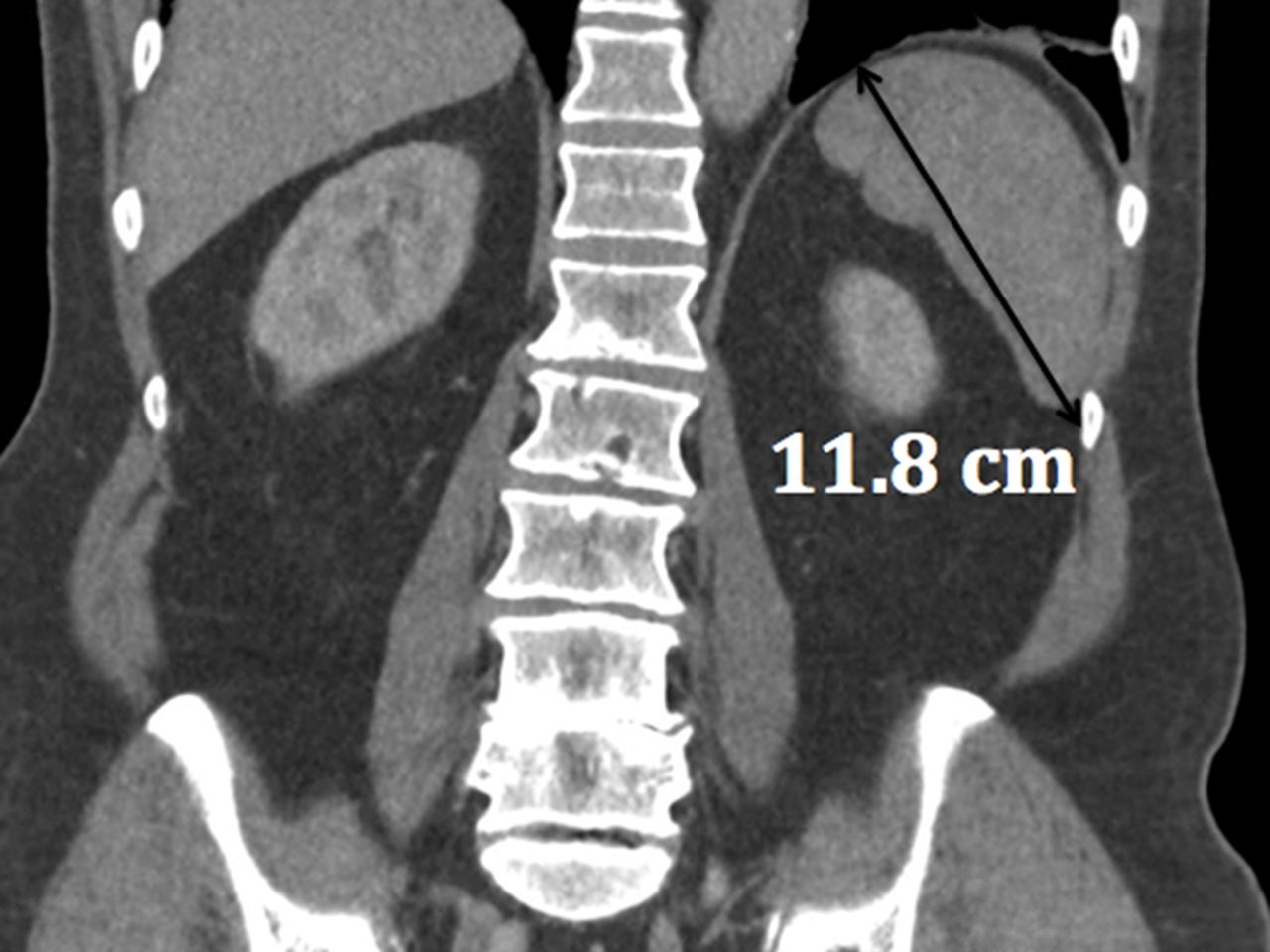
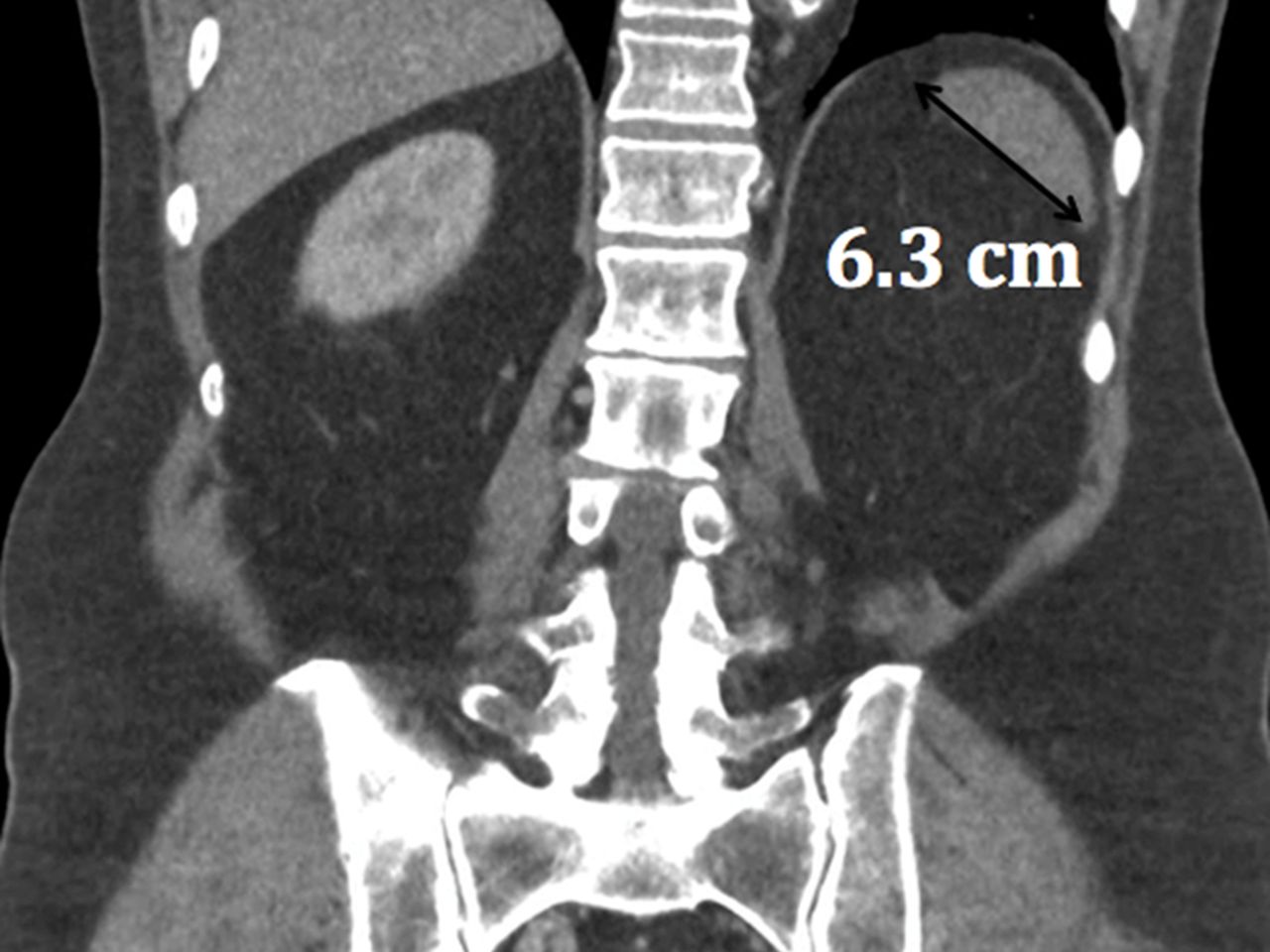
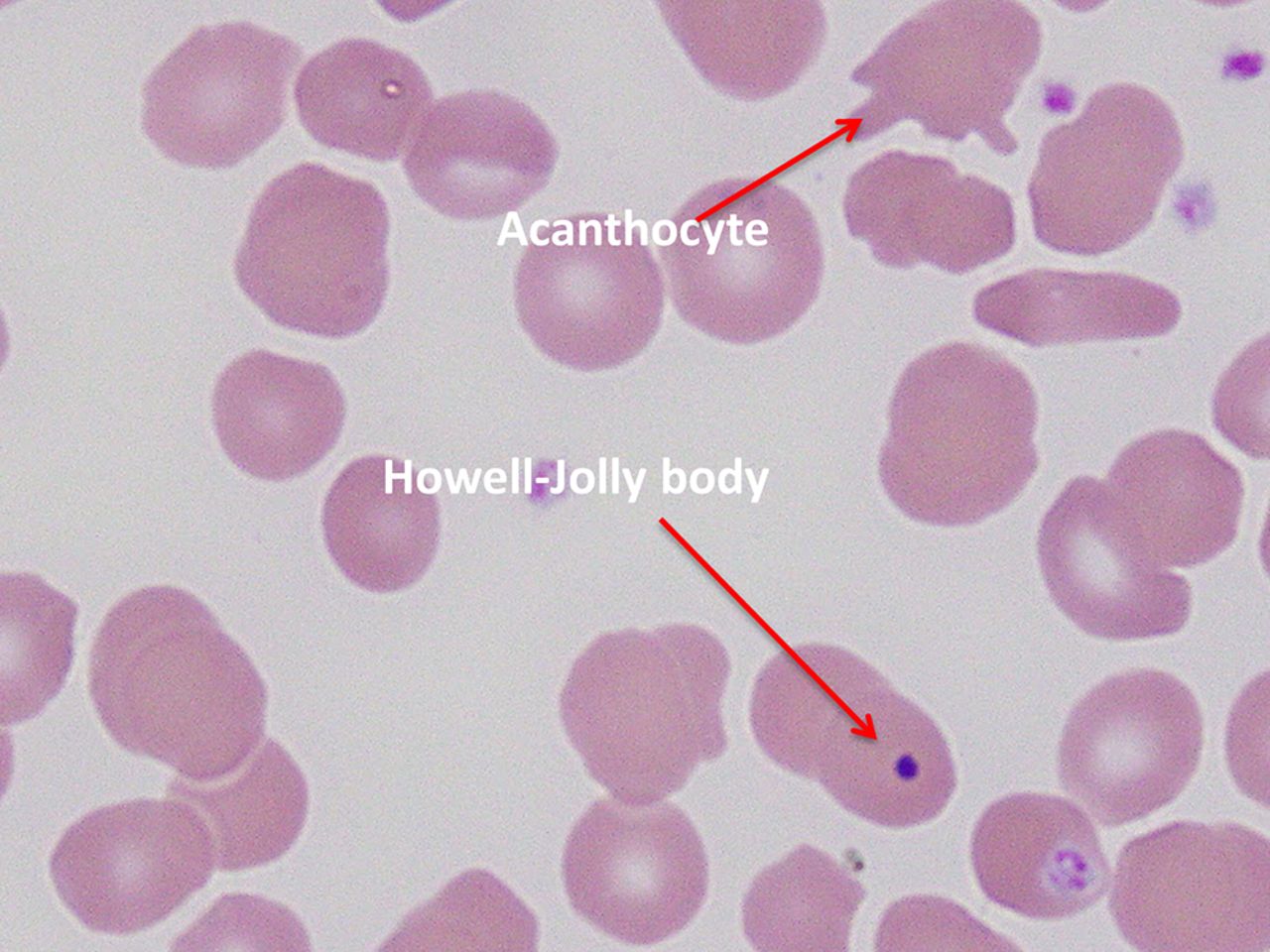
After seven months of immunotherapy, he achieved a complete radiological response to treatment with an accompanying reduction in splenic size (figure 2). Subsequent imaging demonstrated a persistent reduction in splenic size and by June 2015, only a spleen remnant remained (figure 3). Functional hyposplenism was demonstrated with Howell-Jolly bodies and Acanthocytes on the peripheral blood film (figure 4).

Coronal abdominopelvic CT demonstrating a reduction in the splenic length to 6.3 cm.

Coronal abdominopelvic CT with residual splenic remnant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Blood film demonstrating signs of hyposplenism with Acanthocytes and Howell-Jolly bodies.
His treatment was complicated by a range of immune-related adverse events (irAE) including hypophysitis, nephritis and colitis.Although steroid dependant, he remains in radiological remission with an excellent performance status. In the absence of alternative autoimmune pathology, we hypothesise that this is a case of checkpoint inhibitor-induced autosplenectomy, the first reported case of a new rare irAE.
With increasing use of checkpoint inhibitor‘s in oncology, clinical vigilance for rare irAE associated with these agents is required.
Learning points
Checkpoint inhibitors are a form of immunotherapy that have revolutionised the management of melanoma and provide benefit across a spectrum of malignancies.
These new agents bring with them unique immune-related adverse events (irAE).
Adverse events associtaed with checkpoint inhibitors are common, particularly with combination therapy (55% grade 3–4 severity1) and can be potentially fatal.
Rare immune-related adverse events are increasingly being recognised, they can be inflammatory or autoimmune and impact almost any organ.
As checkpoint inhibitors become part of routine clinic practice, it is paramount that all clinicians providing primary and supportive care to oncology patients develop knowledge and experience with these agents and their potential toxicities.
Acknowledgments
Thanks to Dr Marija Borosak and Dr Rachel Wong for their contribution.
Footnotes
Contributors RD and ML contributed to the acquisition, analysis and interpretation of data for the report, as well as drafting the manuscript. MD contributed to the conception of the manuscript including analysis of the images for the case report and contributed to the development of the manuscript. PP contributed to the development of the concept and the design and development of the manuscript. All authors contributed to critical appraisal and revision of the work and approved the final version of the manuscript for publication. Additionally, all authors agree to be accountable for the accuracy and integrity of the final manuscript approved.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.