Article Text

Statistics from Altmetric.com
Description
A man aged 68 years with a known history of squamous cell carcinoma of the lung presented to the emergency room complaining of an acute episode of dyspnoea. His symptoms had resolved on presentation to the hospital. An EKG was obtained, which showed marked ST-segment elevation (STE) in the anteroseptal leads (figure 1A). No prior EKG was available for comparison. The patient denied any chest pain or pressure, and had no evidence of myocardial necrosis by cardiac biomarkers. Nevertheless, he was taken emergently to the cardiac catheterisation laboratory for a presumed diagnosis of STE myocardial infarction (STEMI). He was found to have severe two-vessel coronary artery disease with possible plaque rupture in the mid-left anterior descending artery (LAD) (figure 2). Overlapping bare metal stents were deployed to the LAD. Concerningly, the patient’s right ventricle was noted to be in a fixed motion suggestive of tumour infiltration. A transthoracic echocardiogram was subsequently performed, which demonstrated a large right ventricular mass with involvement of the interventricular septum and pericardium (figure 3). A CT of his thorax showed an anterior mediastinal mass invading the pericardial space, right ventricular free wall and the right ventricular outflow tract (figure 4). Despite the percutaneous coronary intervention, the STE persisted while the serial cardiac biomarkers remained negative (figure 1B). Additionally, the patient also continued to deny any cardiac symptoms. It was later believed that the STE was likely due to tumour infiltration into the right ventricle, and unlikely to be the classic STEMI due to acute coronary syndrome with resultant occlusive thrombus.

(A) EKG on presentation to the hospital, showing ST-segment elevation in leads V1 and V2. (B) Repeat EKG after percutaneous coronary intervention showing persistent ST-segment elevation in leads V1 and V2.

Coronary angiogram showing the left anterior descending artery in both the preintervention and postintervention views from the right anterior oblique with cranial angulation (RAO CRAN) perspective.

Parasternal long-axis view in echocardiogram showing an infiltrating mass in the right ventricle (arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
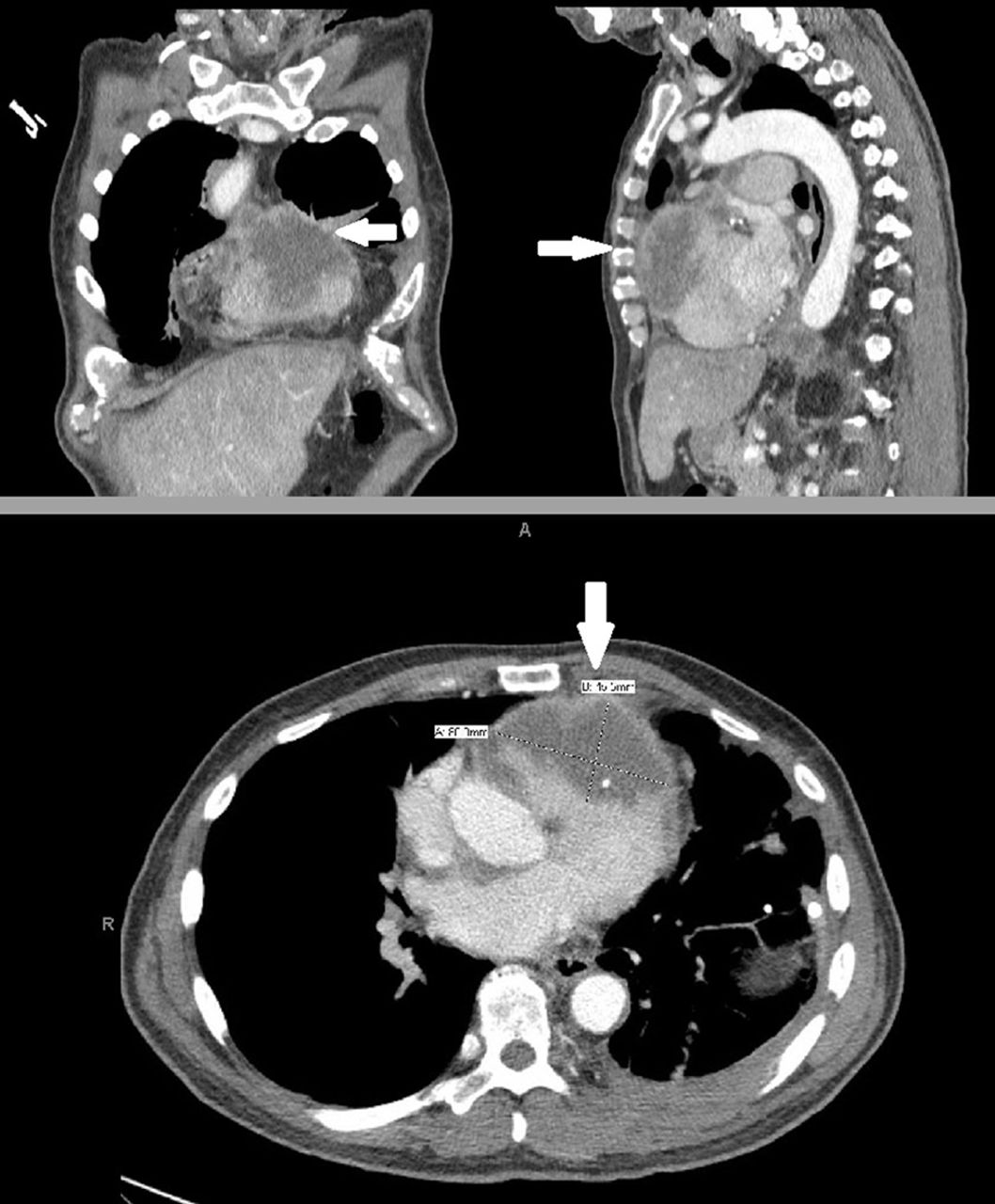
CT of thorax showing tumour infiltration into the myocardium (arrow) in three different views, coronal (top left), sagittal (top right) and transverse (bottom).
The differential diagnosis of STE is broad and extends beyond acute myocardial infarction (AMI). Once AMI is ruled out, other relatively more common considerations include acute pericarditis, Prinzmetal’s angina, hyperkalaemia, left ventricular hypertrophy, left bundle-branch block, Brugada syndrome and pulmonary embolism.1 2 Although relatively rare, STE due to metastatic tumour involving the myocardium had been described in published literature dating five decades back. Although the mechanism of this phenomenon remains unclear, one hypothesis centres around the idea of an injurious current resulting from the inflammation surrounding the tumour, ionic transfer of potassium from necrotic tissue with resultant electropotential difference and neoplastic stretch of adjacent muscle fibres.2 3 In this article, we presented a case of a patient who was initially presumed to have a STEMI based on EKG findings, but was later found to have myocardium compression and infiltration from lung metastasis. He did not have evidence of direct tumour invasion to the LAD on his coronary angiogram. His persistent STE and negative serial biomarkers despite coronary stent placement (as well as absence of angina symptoms) supports this change in diagnosis. Our patient had previously tried palliative carboplatin and paclitaxel with progression of disease. He had been subsequently enrolled in the Lung Cancer Master Protocol (Lung-MAP) trial and had been treated with nivolumab and ipilimumab prior to this admission. Unfortunately, he had continued to demonstrate tumour growth and had been ultimately switched to gemcitabine for a brief moment without improvement. Given his overall disease progression and poor prognosis, the patient declined additional chemotherapy during this admission and wished to pursue hospice care. He passed away 2 weeks later.
Learning points
The differential diagnosis of ST-segment elevation is broad, but the most important and time-sensitive diagnosis to consider is acute myocardial infarction.
If a patient with known malignancy presents with an isolated ST-segment elevation without a clinical presentation suggestive of acute coronary syndrome, tumour compression and/or infiltration of the myocardium should be considered in the differential diagnosis.
Footnotes
Competing interests None declared.
Patient consent Consent obtained from next of kin.
Provenance and peer review Not commissioned; externally peer reviewed.