Article Text

Summary
Successful total scalp replantation was performed in our case. Based on the angiosome concept and anatomical study, the avulsed scalp survived with unilateral anastomosis of the superficial temporal artery and superficial temporal vein, largely due to the presence of rich arterial and venous arcades in the scalp. The patient currently has no problems with activities of daily living, although total hypoaesthesia and dysfunction of the left frontal muscle of the forehead are present. In addition, the combined findings of hair growth pattern indicated the vascular territories of the scalp skin.
- vascular surgery
- plastic and reconstructive surgery
- orthopaedic and trauma surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Total scalp avulsion is a rare injury, mostly occurring during industrial accidents. Microsurgical replantation is the optimal treatment. Composite grafting or free flap transfer may fail to satisfy aesthetic and functional demands.1–3 We herein describe a patient who underwent microvascular replantation and showed an interesting postoperative hair growth pattern.
To our knowledge, this is the second reported case of successful treatment of total scalp avulsion in Japan.
Case presentation
A 64-year-old woman sustained total scalp avulsion when her long hair was pulled into a spinning machine. She was not wearing a helmet (figure 1). The avulsion started from the top of the nose, crossed the upper one-third of both ears and extended down to the lower occipital area. Neurological examination revealed intact bilateral extraocular muscle and normal facial sensory responses.

Entire avulsed scalp after hair was shaved.
Emergent replantation of the avulsed scalp was performed under general anaesthesia, with an interval between the injury and revascularisation of 4 hours (figure 2). The right superficial temporal artery (STA) and superficial temporal vein (STV) had sufficient length, with STA diameter of 1.0 mm and STV diameter of 1.1 mm, enabling direct anastomosis. Immediately after anastomosis of the right STA and STV, abundant blood supply was noted throughout the entire scalp, including the left temporal area, with perfusion from the circumferential edge. The left STA and STV were narrow and short, and additional anastomosis resulted in much less blood flow without use of a vein graft. Four drains were inserted in the occipital space between the scalp and skull. We did not use thrombolytic drugs during and after surgery. Postoperative congestion occurred with concomitant effusion between the epicranial aponeurosis and skull; however, the symptom improved gradually with the aid of drains.

View of the head in the emergency room. Top of the head shows the pericranium; the frontal and temporal fascia can be seen.
The scalp mostly survived; however, partial skin necrosis (3.0×4.0 cm2) developed in the lower left occipital region. Therefore, the lesion was debrided and reconstructed with a split skin graft 2 weeks after the operation. The wound healed well, and thick hair growth was clearly observed. As of 2 months after the first operation, exuberant hair was evident (figure 3). Another finding was that the patient’s hair growth pattern was different between the sides, that is, the right temporal area had greater hair growth compared with the left. At 1 year postoperatively, her hair had grown sufficiently, and right eyebrow movement was observed (figure 4A,B). Although sensory paralysis and dysfunction of the left frontal muscle remained, the patient was very satisfied with the aesthetic result.

Two months postoperatively, hair growth was evident. Partial skin necrosis (3.0×4.0 cm²) developed in the lower left occipital region; this was debrided and reconstructed with a split skin graft 2 weeks after the operation. Right temporal area has luxuriant hair growth, compared with the left occipital area.

Frontal view. At 1 year postoperatively, her hair had grown sufficiently, and right eyebrow movement was observed. There was no difficulty in opening and closing the eyelids. (A) Frontal view, eyes opened. (B) Frontal view, eyes closed.
Outcome and follow-up
The wound healed well, and thick hair growth was clearly observed. As of 2 months after the first operation, luxuriant hair was evident (figure 3). Another finding was that the patient’s hair growth pattern was different between the sides, that is, the right temporal area had greater hair growth compared with the left. At 1 year postoperatively, her hair had grown sufficiently, and right eyebrow movement was observed (figure 4A,B).
Discussion
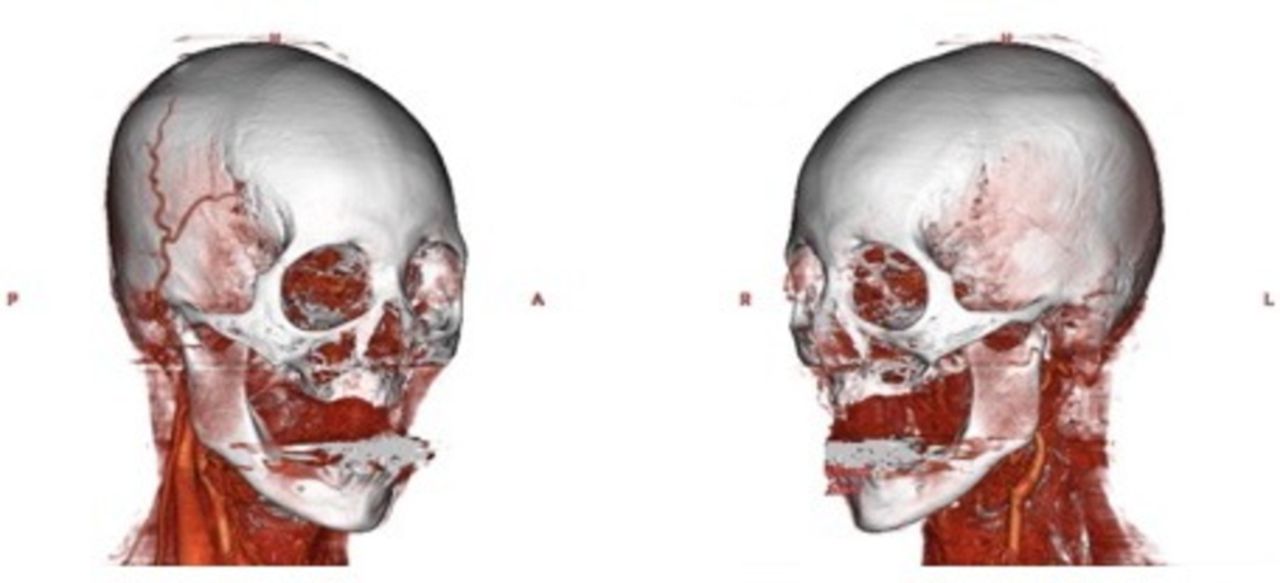
Microvascular replantation of an avulsed scalp was first described by Miller et al in 1976.4 Since then, many authors have recommended anastomosis of two or more arteries and as many veins as possible.2 3 However, some clinicians have demonstrated that the scalp, and up to two-thirds of the face, can be successfully restored using only one artery.1 5 In our case, partial skin necrosis only developed in the left lower occipital area. Additionally, as demonstrated by three-dimensional CT angiography 4 months, postoperatively (figure 5A,B), only the right STA and STV showed blood flow, while the left STA and STV could not be enhanced after contrast medium injection, suggesting the entire scalp had circulation via the right STA and STV, with occlusion on the left side. These findings may reflect the superior left postoperative hair growth pattern.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contrast-enhanced three-dimensional CT angiography (figure 4) months after the operation. On the lateral view, the right superficial temporal artery and vein are enhanced and clearly delineated. However, the left superficial temporal artery and vein were not delineated. (A) Right angle. (B) Left angle.
According to the angiosome concept, the body is composed of multiple three-dimensional composite blocks of tissue supplied by particular source arteries or ‘vascular territories’. Therefore, a transferred or replanted flap or tissue survives within two vascular territories from the vascular pedicle by perfusion via opened choke vessels or true anastomosis between the territories.6 7 There are rich arterial and venous arcades in the subcutaneous layer above the galea aponeurotica, including bilateral superficial temporal, occipital, posterior auricular, supraorbital, supratrochlear and dorsal nasal vessels.7 8
Anatomical studies and the angiosome concept predict the reliability of blood circulation and survival of the entire scalp with anastomosis of a single artery. However, skin necrosis in the left occipital area in our case was thought to be due to a distance of more than two anatomical territories removed from the source territory (right superficial temporal area).
No nerves could be repaired in our case, but sensation from the frontal to parietal region recovered at 1 year postoperatively. Some researchers stated that in partial scalp replantation cases, sensory recovery is expected even without nerve anastomosis.9 10 The frontal muscle resumed contraction 6 months after the operation. Follow-up observation has been continued, with attention to further neural recovery.
Consequently, anastomosis of the unilateral STA and STV will nourish almost all the replanted scalp. However, to encompass the entirety of the scalp required inclusion of the occipital artery within the scalp.
To our knowledge, this is the second reported case of successful treatment of total scalp avulsion in Japan, following the first reported case of Okada et al.10
Patient’s perspective
I was very satisfied with the aesthetic result. I have no problems in daily life activities.
Learning points
This report provides additional proof that a totally avulsed scalp can be salvaged with anastomosis of one artery and vein in cases where multiple arterial anastomoses are not possible.
Scalp avulsion is uncommon in clinical practice; however, when it does occur, the outcome depends on microsurgery.
The mixed hair growth pattern reflected the vascular territories of the scalp skin.
Footnotes
Contributors Both authors contributed to the planning, conduct and reporting of the work described in the article.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.