Article Text

Statistics from Altmetric.com
Description
Meningitis is an inflammatory syndrome involving the meninges, and it manifests with headache and stiff neck. On the contrary, encephalitis refers to the inflammation of the brain parenchyma. The causative pathogens can be manifold though, except for immunocompromised patients; in literature, there are no cases of meningoencephalitis caused by bacteria usually present in the bowel.
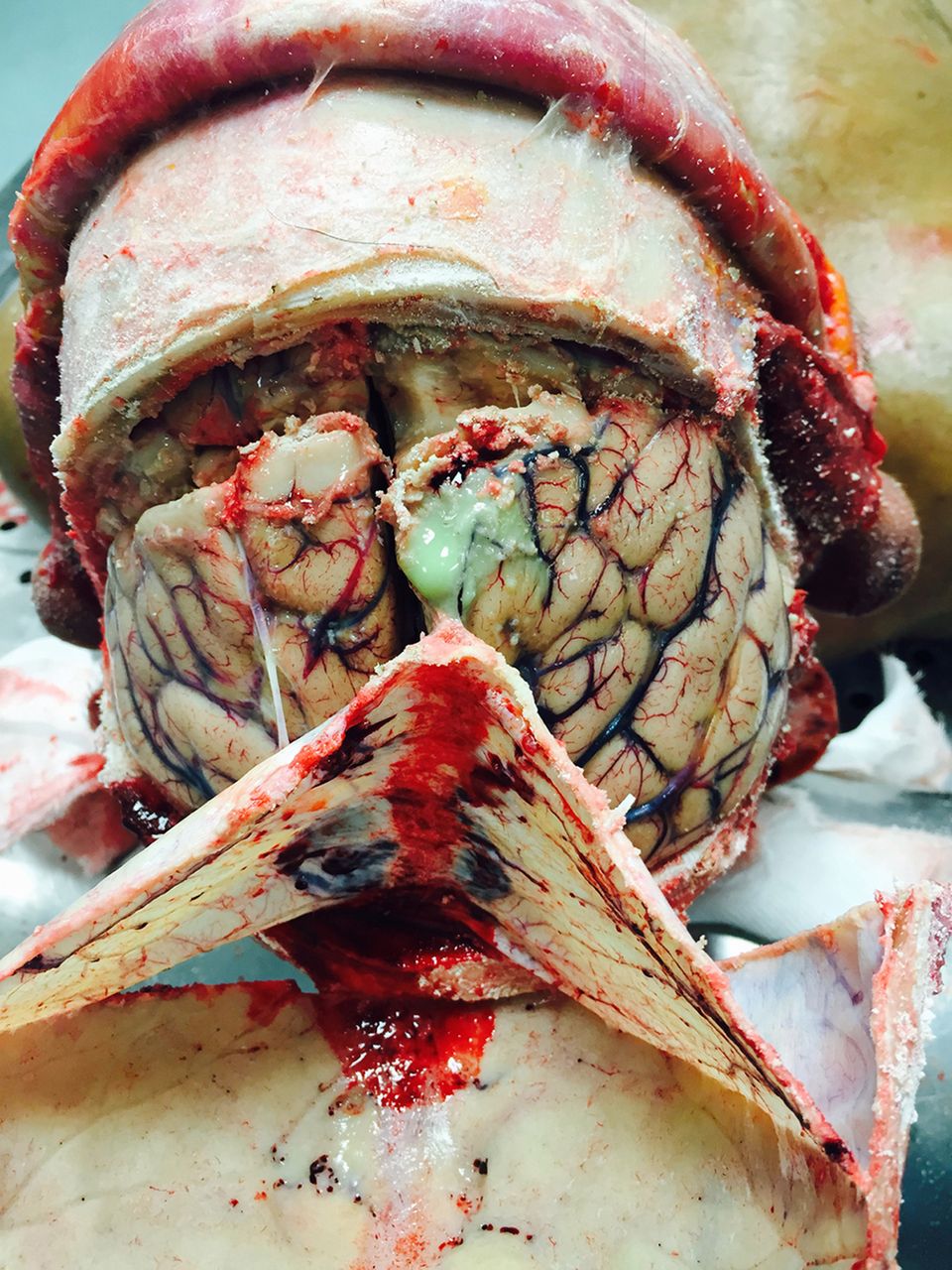
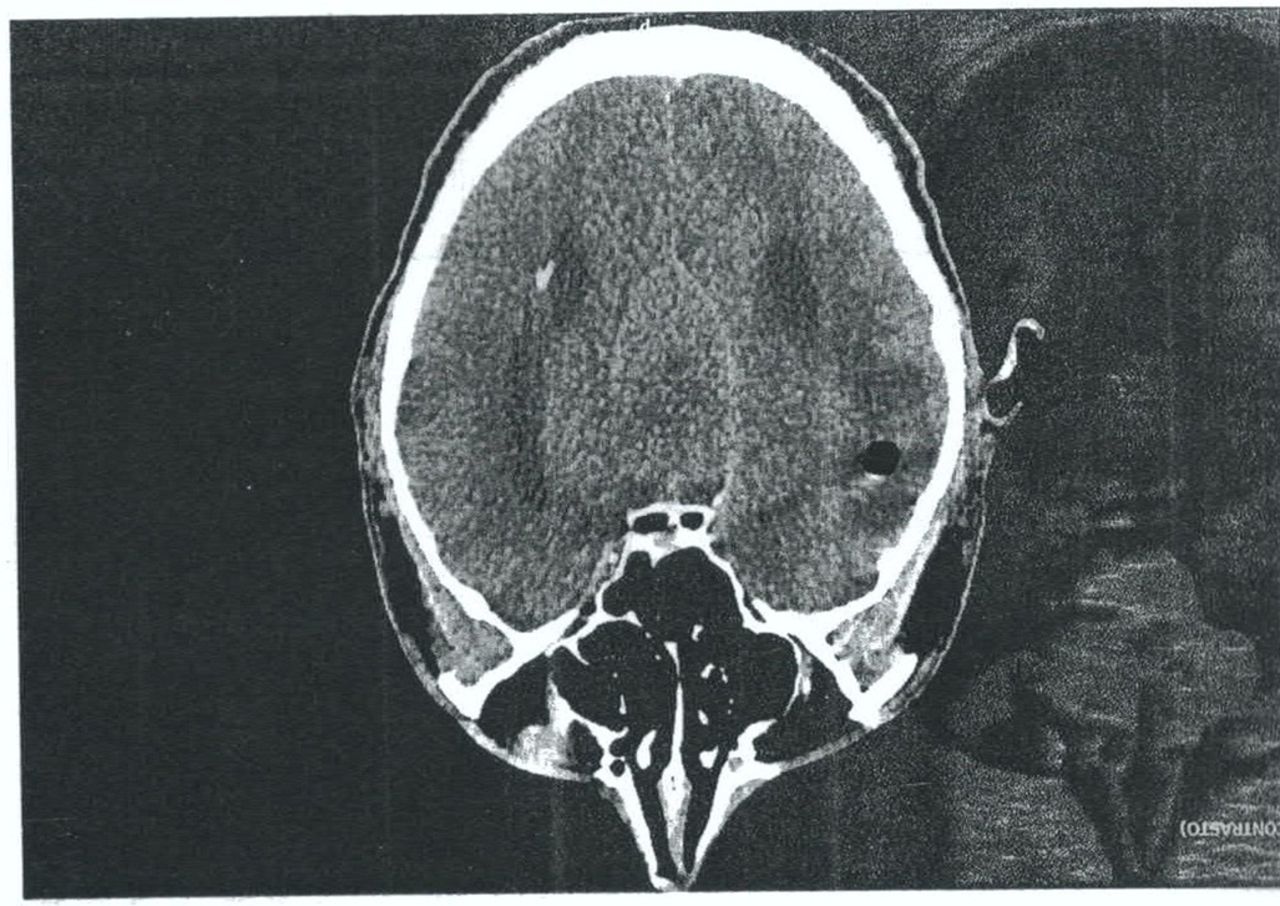
We report the case of a 40-year-old man. Following an earache, the man went to the hospital. In anamnesis, the man reported a chronic otitis media for many years, and clinicians, noting auricular bleeding, advised local antibiotic treatment. The next day, he had fever, treated with paracetamol. After 3 days, following the worsening of the clinical condition, the man returned to the hospital where physicians detected temporal and spatial disorientation, neck stiffness and fever of 39.5°C. Despite medical therapy, the man died after a few hours. An autopsy was performed. It showed an abscess on the right fronto-parietal lobe (figure 1) and, on the cerebellar vermis (figure 2), a thrombosis of the lateral sinus and a massive septic thromboembolism (figures 3 and 4) of pulmonary veins, the superior vena cava, aorta and right iliac vein. An histopathological and microbiological investigation was carried out.1 In particular, the microbiological investigation of the brain and the meninges (made with sterile swabs) showed the presence of Escherichia coli, Enterobacter cloacae complex, Acinetobacter baumannii and Candida albicans. The histopathological investigation after autopsy showed granulocyte infiltrate with presence of polymorphonucleates in fibrin agglomerates. During hospitalisation, the man have presented a marked neutrophilia with increase of lymphocytes and monocytes. The CT showed the presence of right cerebral air bubble with diffuse oedema and hyperdense area of the inner ear (figure 5).

Brain abscess on the right fronto-parietal region.

Abscess on the cerebellar vermis.

Finding of pulmonary thromboembolism.

Septic thromboemboli found in the inferior vena cava, the iliac vessels and the heart.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT scan showed right cerebral air bubble with diffuse oedema and hyperdense area of the inner ear.
Chronic otitis media may present extracranial and/or intracranial complications. The most common extracranial diseases include facial paralysis, subperiosteal abscess, mastoiditis and labyrinthitis. The intracranial complications are meningitis, brain abscess, lateral sinus thrombosis, extradural abscess, hydrocephalus and encephalitis. Many studies have shown that the high incidence of otitis media, the inaccuracies in the diagnosis and the possibility of life-threatening sequelae make this disease a major public health problem. As such, the physician should have a high index of suspicion during the medical examination of a patient with otitis media.2 3
Although it is often problematic to determine the path of bacterial infection from the middle ear to the meninges in the presence of middle ear otitis, possible paths are (1) via the blood, (2) direct spread or invasion (3) through the bone defect and (4) through the cochlear aqueduct.
Thus, if there is an external invasion, it is easy that the causative bacteria could be different with respect to the microorganisms usually responsible for the meningitis. The purpose of the study is to emphasise the role of diagnosis and treatment of otitis media in prevention of fatal events, in particular in the presence of tympanic perforation. The case has confirmed that, as a result of bathing diving in contaminated water, the entrance through the right ear allowed the access of bacteria usually present in the faeces.
Learning points
Tympanic perforation is a risk factor for migration of external pathogens within the meninges.
It is an erroneous but widespread belief that the intracranial complications of acute and chronic otitis media belong to the past or they are attributable only to the developing countries.
This case has shown that, despite the improvements in antibiotic treatment, the problem of morbidity and mortality remains high.
Footnotes
Contributors IA is the forensic pathologist and the official responsible of the case. She performed the autopsy, conceived the idea and managed the whole realisation of the paper. SG has contributed through the realisation of microbiological analysis and the interpretation of the data. MAS has contributed through the writing of the case report. PR managed with her the realisation of the work.
Competing interests None declared.
Patient consent We certify that this study analyzes a patient who died. For this reason it was not possible to obtain consent form. Dr. Aquila I. (Corresponding author) has had an assignment by the prosecutor to carry out an autopsy and for this reason the authors asked permission to court in order to use the case and its scientific data.
Provenance and peer review Not commissioned; externally peer reviewed.