Article Text

Statistics from Altmetric.com
Description
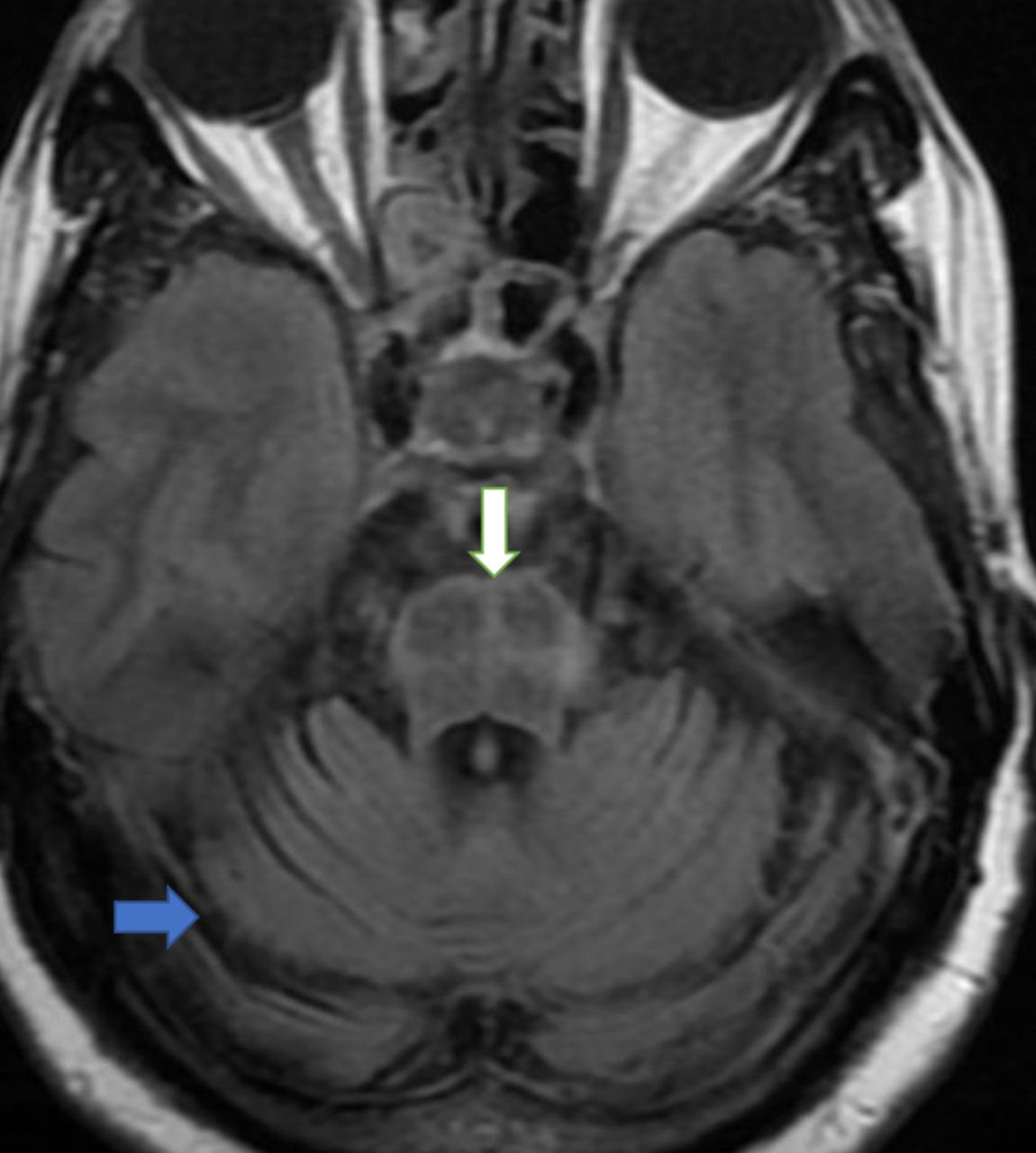
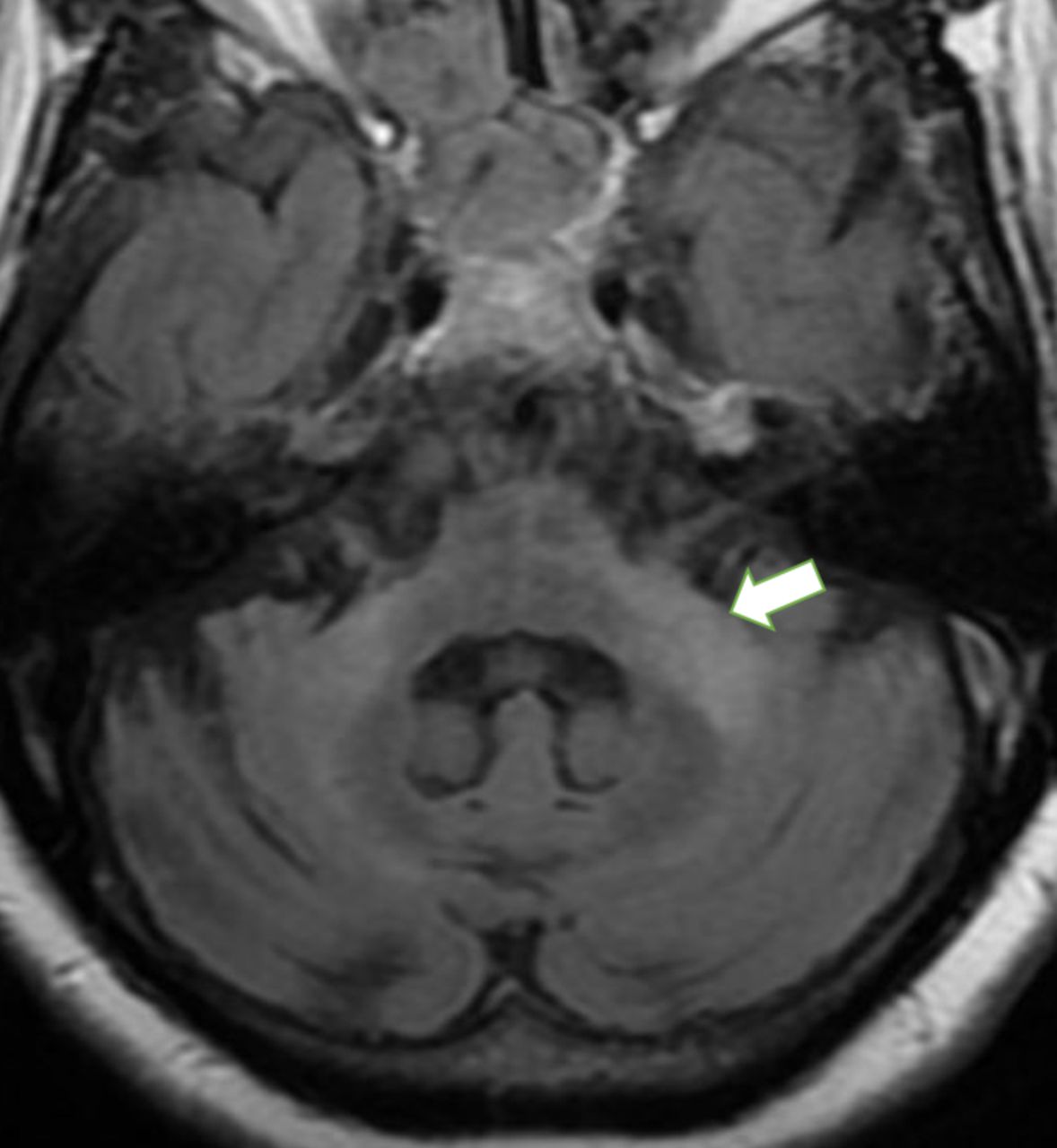
A 52-year-old female patient presented with progressive gait unsteadiness for 6 months. Over the months, it has worsened to such an extent that she required support for walking. She also complained of frequent episodes of light-headedness on standing up from lying down or sitting down. She had no urge incontinence, urinary retention, increased frequency of micturition or constipation. She had no bradykinesia, rigidity, memory loss or features suggestive of dementia. There was no family history of similar complaints or dementia. On examination, she was found to have gait ataxia, nystagmus and intention tremors. The gait was broad based with sway towards left side. Her eye movements showed dysmetric saccades and jerky pursuit. She was also found to have postural hypotension. Her supine blood pressure was 170/90 mm Hg and her standing blood pressure was 140/70 mm Hg. She had no resting tremor, rigidity or bradykinesia. Babinski’s sign was negative. Deep tendon reflexes were normal. Her speech was normal. Her mental status examination was found to be within normal limits. A provisional clinical diagnosis of probable multiple system atrophy (MSA) was made. MRI brain study was performed, which showed cruciform hyperintense signal in the pons in T2 fluid-attenuated inversion recovery (FLAIR) images—hot cross bun sign (figure 1). T2 FLAIR hyperintensity of bilateral middle cerebellar peduncles (MCPs) was also noted, which is known as bright MCP sign (figure 2). There was significant cerebellar atrophy (figures 1 and 2). The putamen showed no e/o atrophy or signal changes. There was no significant cerebral cortical atrophy. There was no postvoid residue on a urinary bladder ultrasound scan. Based on the history, clinical examination and imaging findings, a diagnosis of probable MSA cerebellar type (MSA-C) was made.

Axial T2 FLAIR image showing cruciform hyperintensity in pons and cerebellar atrophy.

{kind=link}
{kind=link}
Axial T2 FLAIR image showing atrophy with high signal intensity in bilateral middle cerebellar peduncle. Cruciform hyperintensity in pons and cerebellar atrophy are also noted.
Multiple system atrophy is a neurodegenerative disorder that is classified under Parkinson plus syndromes with variable involvement of the basal ganglia, pontocerebellar region and the autonomic system. Striatonigral degeneration, olivopontocerebellar atrophy and Shy-Drager syndrome are now considered as part of MSA.1 The histopathological hallmark of MSA is accumulation of α-synuclein within glial cytoplasmic inclusions.2 Based on clinical features, MSA is classified into MSA-P with predominant parkinsonism symptoms and MSA-C with predominant cerebellar and autonomic symptoms.3 Our patient presented with cerebellar ataxia and on examination was also found to have autonomic disturbance in the form of postural hypotension. MRI brain in patients with MSA-C show significant pontocerebellar atrophy with prominent fourth ventricle.1 Cruciform T2/T2 FLAIR hyperintensity is also noted in the axial sections of pons due to selective loss of myelinated transverse pontocerebellar fibres and neurons in the pontine raphe. This is known as the hot cross bun sign. High T2/T2 FLAIR signal intensity with volume loss is also noted in the middle cerebellar peduncles, which is known as the bright MCP sign.4 Our patient had both hot cross bun sign and bright MCP sign. The putamen in our patient showed no atrophy or T2 hypointense signal seen in MSA-P.3 The differential diagnosis of hot cross bun sign include MSA, spinocerebellar ataxia type 2 and type 3 (younger age of onset, associated with polyneuropathy, the myelinated transverse pontocerebellar fibres are preserved as compared with MSA-C) and Parkinsonism due to vasculitis (significantly higher load of subcortical white matter lesions).5 The bright MCP sign can also be seen in Wallerian degeneration post pontine infarct/demyelination (gliosis in pons), fragile X tremor ataxia syndrome (involvement of splenium of corpus callosum and white matter lesions in cerebrum) and toluene abuse (periventricular white matter signal changes, thalamic hypointensity and cerebral atrophy).6 In the right clinical setting, a combination of hot cross bun sign and bright MCP sign should confirm diagnosis of probable MSA-C. The definite diagnosis can be made only on histopathological examination.7
Learning points
Hot cross bun sign and bright middle cerebellar peduncles sign are seen in multiple system atrophy (MSA) cerebellar type.
MRI is an invaluable tool in characterising MSA.
Even though clinical symptoms and signs raise suspicion of neurodegenerative disorder, imaging helps in confirming the diagnosis.
Footnotes
Contributors SC: analysis and interpretation of the case. FF: conception and design. AB: acquisition of images and clinical data. BP: proof reading, verification and final approval.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.