Article Text

Statistics from Altmetric.com
Description
A 59-year-old asymptomatic woman presented for follow-up CT thorax, abdomen and pelvis (CT-TAP). Fifteen months previously she underwent a left radical nephrectomy for a T1bN0MO, 5.5 cm Fuhrman grade 4 clear cell renal cell carcinoma (CCRCC) (figure 1).
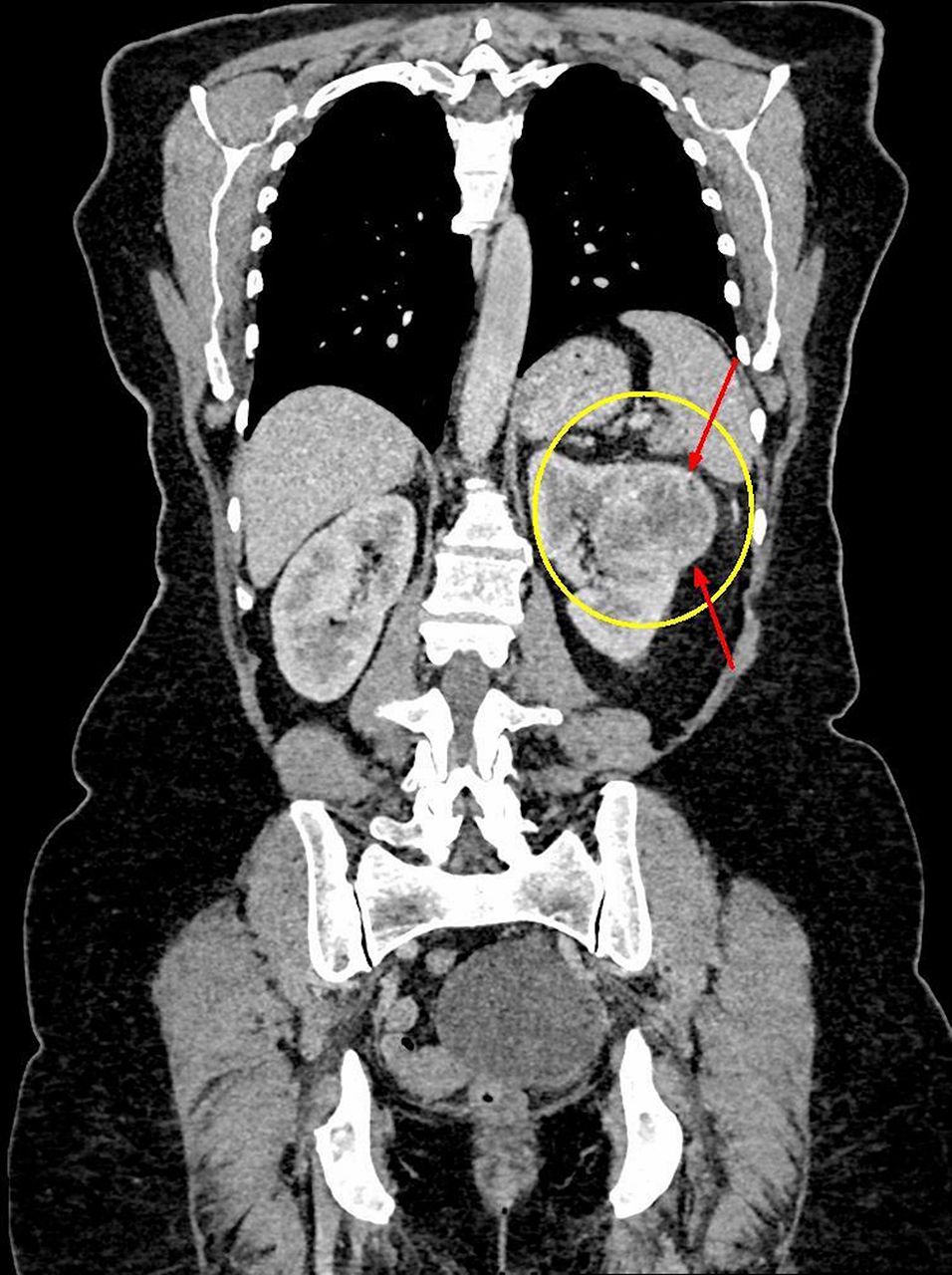
Portal venous phase coronal image CT-TAP. The 6.8 cm expansile, heterogenous lesion is centred in the renal cortex of the mid/upper pole of the left kidney (yellow circle). It appears well encapsulated (red arrows) and abuts the renal sinus with no clear invasion. The low attenuation may be due to necrosis or cystic components. CT-TAP, CT thorax, abdomen and pelvis.
The CT-TAP revealed a new 3.6 cm peripherally enhancing, centrally necrotic, intramural lesion in the fundus of the stomach (figure 2). It was decided to biopsy the lesion via oesophago-gastro duodenoscopy (OGD). It was not apparent on direct visualisation of the stomach mucosa, thus confirming its submucosal location. In light of its location, as well as the onset of upper gastrointestinal symptoms, lack of histological diagnosis or evidence of metastatic disease, a laparoscopic sleeve gastrectomy was performed. A tan intramural mass in the fundus of the stomach was revealed with a similar macroscopic appearance to the primary CCRCC (figure 3). H&E staining revealed tumour cells with a nested pattern of arrangement with clear cytoplasm and prominent nucleoli, classic and identical to the primary CCRCC (figure 4).

Portal venous phase coronal image CT-TAP 15 months later. New 3.6 cm centrally necrotic, intramural, peripherally enhancing lesion in the fundus of the stomach. Note absent left kidney secondary to previous nephrectomy. Small bowel mesentery lies in the left renal fossa.
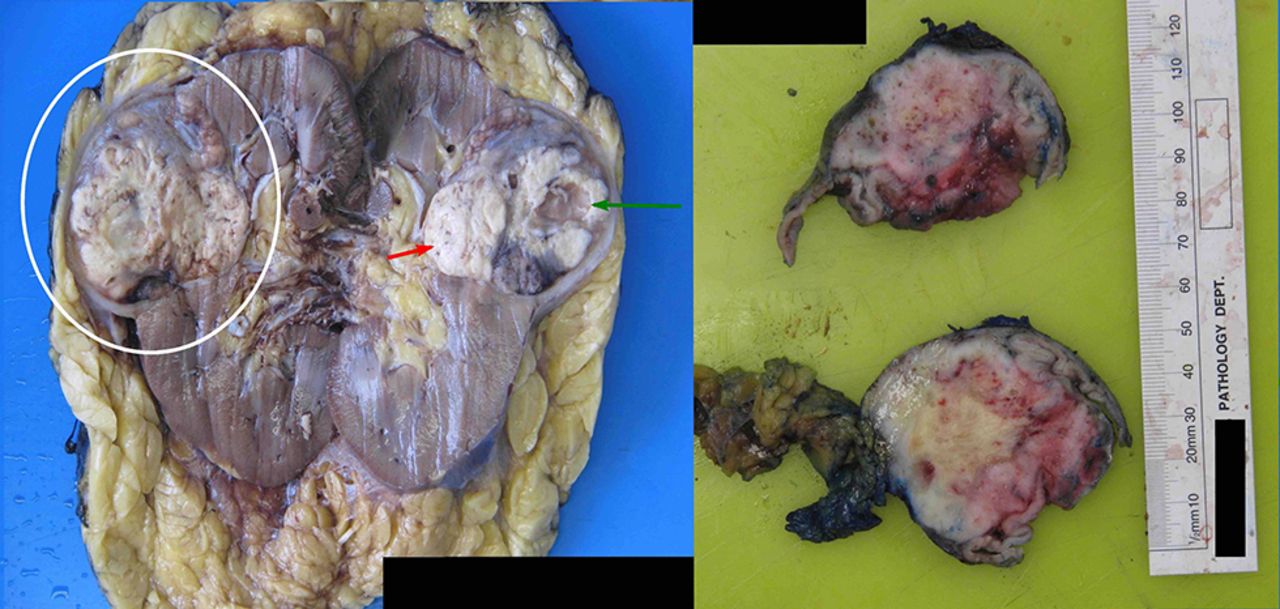
This is a comparison between the resected primary left kidney (left) and the intramural metachronous stomach lesion (right). The kidney has been bivalved to reveal a large, well-circumscribed tumour with a variegated tan/yellow cut surface (red arrow) and a prominent cystic area, responsible for the heterogenous appearance at CT (green arrow). Note the overall similar gross appearance to the sleeve gastrectomy specimen. Normal stomach mucosa is adjacent to the ruler.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
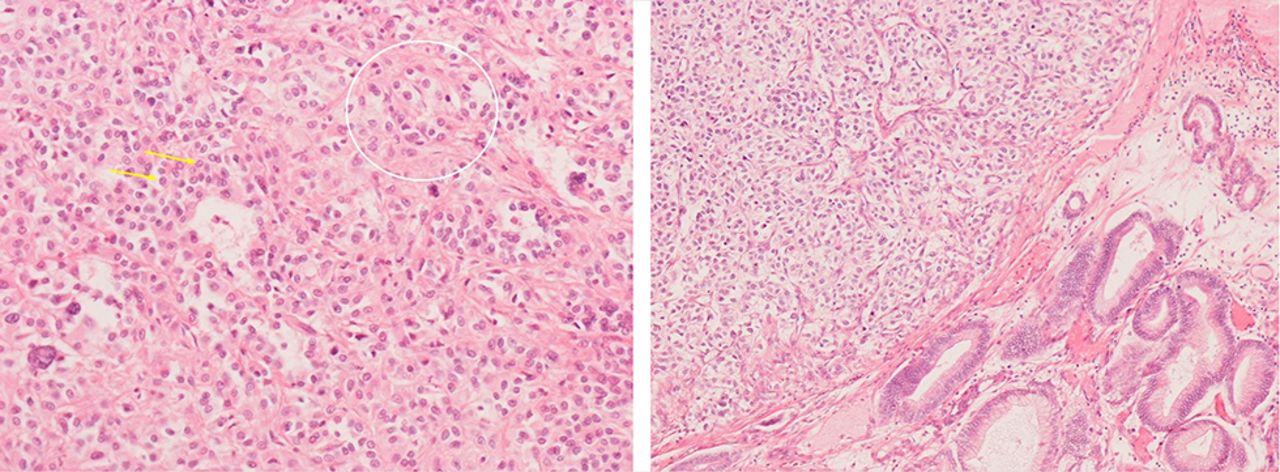
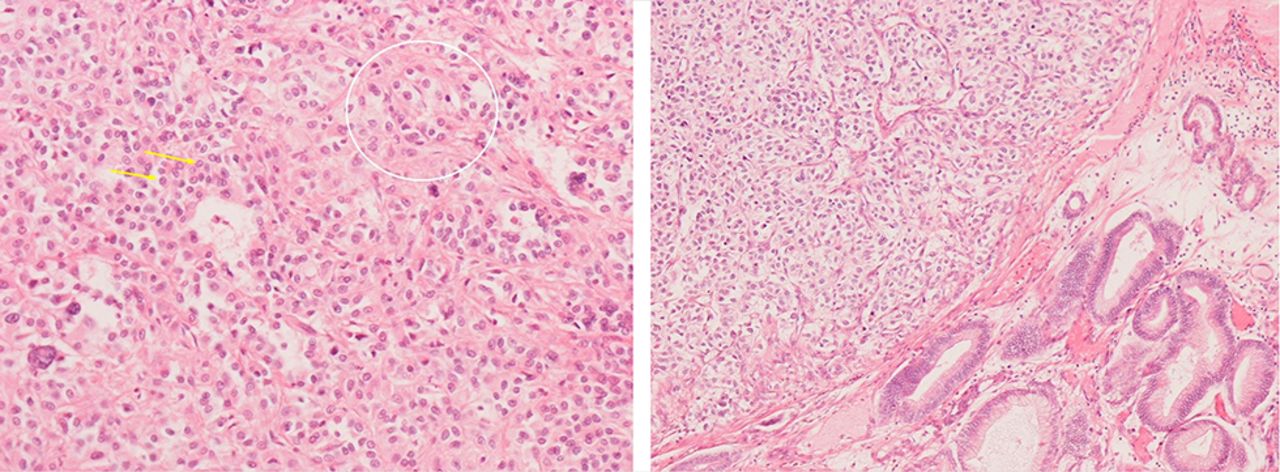
Low power H&E stain of the primary CCRCC (left) and the stomach lesion (right). The tumour is composed of nested polygonal cells with predominantly small round nuclei (yellow arrows) and the classic vacuolated cytoplasm of CCRCC (example illustrated by white circle). Note the identical pattern in the resection specimen. Normal gastric mucosa is demonstrated on the right of the image. CCRCC, clear cell renal cell carcinoma.
The annual incidence of renal cell carcinoma (RCC) has risen in the USA and Europe by 3% per year during the last several decades. Approximately 20% of patients will have metastatic disease at the time of diagnosis with 50% developing metachronous metastasis post nephrectomy.1 CCRCC is known for unusual sites of metastatic spread and can typically involve the lung, bones, liver, lymph nodes or adrenal glands. A metastasis from any cause to the stomach is exceedingly rare and can account for between 0.3% and 0.8% of all gastric neoplasia.2 Such is the rarity of gastric metastasis from all histological subtypes of renal cell carcinoma, there are only approximately 25–30 cases described in the literature. The largest case series is of five patients over a 21-year time period in 2082 patients.3 This is the best current level of prognostic evidence for gastric RCC metastases, which usually presents late in the disease process. The majority of patients show concomitant tumour spread to other organs with poor outcome. Our patient has subsequently developed peritoneal metastases and is being treated with sunitinib, an inhibitor of receptor tyrosine kinase.
Learning points
Renal cell carcinoma (RCC) is known for unusual sites of metastatic disease with virtually any organ being involved. A solitary metastasis to the stomach is exceedingly rare.
Case series is the best current level of prognostic evidence for gastric RCC metastasis and is associated with a poor outcome.
Clear cell renal cell carcinoma (CCRCC) histologically is typically characterised by nested polygonal cells interspersed with intricate, arborising vasculature with predominantly small round nuclei and classic vacuolated cytoplasm. Diagnosis of metastatic CCRCC is usually achievable by routine histological examination alone.
Footnotes
Contributors MKO’R was involved in the conception, data acquisition, writing and design of the manuscript. GS, KH-S and HF were involved in the conception, writing and editing of the manuscript. All authors have reviewed the final version and approved it.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.