Article Text

Statistics from Altmetric.com
- endocrinology
- diabetes
- drugs: endocrine system
- healthcare improvement and patient safety
- medical education
Description
A 15-year-old boy with a 3-year history of type 1 diabetes mellitus was referred to endocrinology clinic for the management of uncontrolled blood glucose levels. His present treatment plan comprised subcutaneous basal-bolus insulin regimen. He was taking regular insulin before the three major meals and insulin glargine at the bedtime. His body mass index (BMI) was 14.8 kg/m2 and HbA1c level 14.9%, suggesting uncontrolled hyperglycaemia for a long time.
On examination, he was found to have remarkably prominent bilateral lipohypertrophic areas on the lower abdomen (figure 1), large enough to be noticeable even through the clothing.

Showing prominent bulge on either side of the lower abdomen (side view).
His injection practices revealed that he was self-administering insulin over the abdomen with the syringe of needle size 6 mm, apparently leading to intramuscular injection in a thin-built person.1 Furthermore, he was drawing his recommended dose of basal insulin with the 40 IU/mL syringe out of a vial of 100 IU/mL strength resulting into 2.5 times of the prescribed amount. However, the match between insulin syringe and strength was appropriate for the bolus doses.
He was injecting in the area measured to be around 8.5×5.5 cm on either side of the lower abdomen approximating the size of a credit card. He preferred this area, as injections at this site were painless. In addition, he was not performing systematic site rotation within a quadrant of abdominal area by leaving a space of 1 cm for the subsequent injections. Moreover, one syringe was reportedly used on an average six times. Missing the doses of insulin along with the habit of injecting into lipohypertrophic lesions caused one episode of diabetic ketoacidosis requiring hospitalisation 2 weeks prior to this visit.
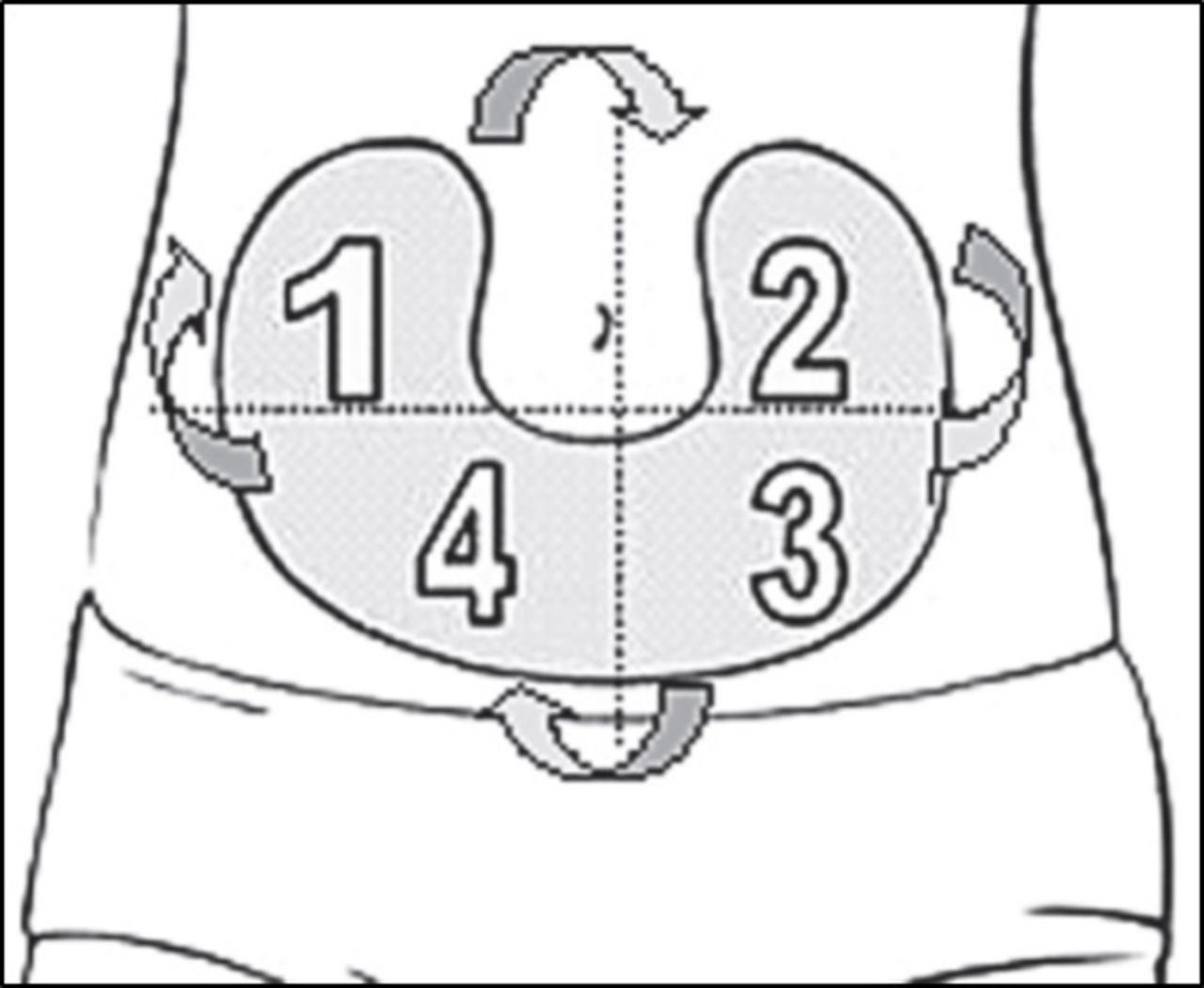
Patient was managed using talk, inspect and educate strategy followed by our endocrinology clinic considering the high prevalence of insulin-related lipohypertrophy in Indian patients.2 Readdressing correct injection technique is very important to curb lipohypertrophy and its consequences. Therefore, the systematic rotation (figure 2) and practice of injections in larger area were explained to the patient. He was also directed to discontinue injections into lipohypertrophic lesions and advised to inject into the normal tissue. It was further recommended to reduce the dose of insulin, guided by self-monitoring of blood glucose, for avoiding hypoglycaemia while shifting to normal site. Patient was educated about the importance of adhering to insulin, appropriate match of insulin strength with syringe and single-time needle use. In view of the low BMI, he was switched to 4 mm needle size available for using with pen device.1
{kind=link}
{kind=link}
Illustration of systematic rotation scheme within abdominal quadrants. One quadrant per week in clockwise manner and then moving to the next quadrant. (Photographs courtesy of Lourdes Saez-de Ibarra and Ruth Gaspar, Diabetes Nurses and Specialist Educators from La Paz Hospital, Madrid, Spain.)
Learning points
Create TIE (Talk, Inspect and Educate) with the patient
Talk to the patients and their families regarding diabetes management to understand the ongoing challenges faced by them.
Inspect the injection sites on regular basis for the early detection of lipohypertrophy.
Educate the patients and their families about importance of proper insulin injection practice.
Footnotes
Contributors Anjana Barola and Pramil Tiwari prepared the manuscript and helped in patient education. Anil Bhansali identified the case, edited the manuscript and guided the clinical management.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.